
Index and Table of Contents
174 Cases with Videos
3 Cases with Images
2 Snippets
5 Lectures
4 Cases of the Day (CODs)
New Onetime Lifetime Subscription
 Bhavin Jankharia
Bhavin Jankharia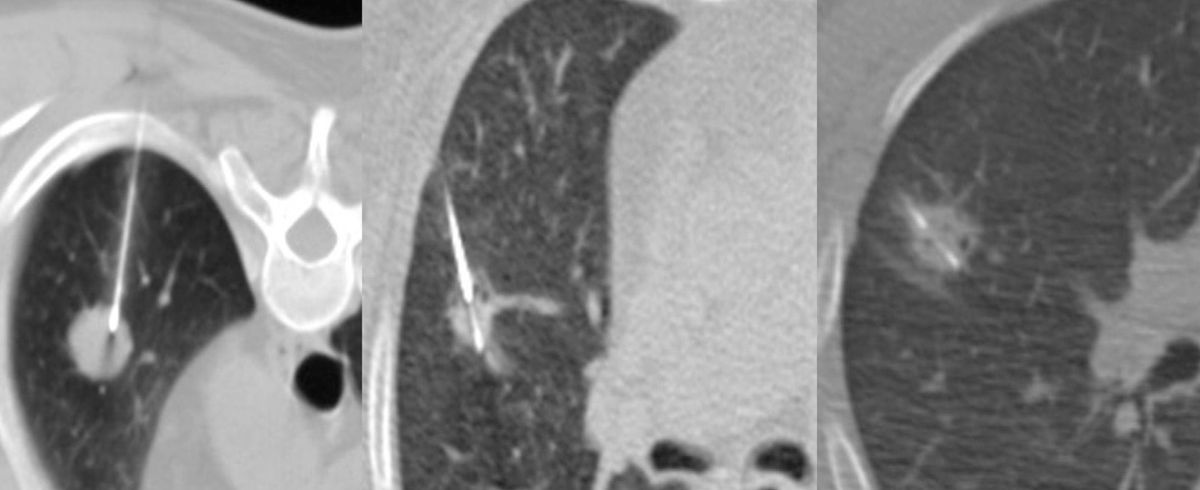
Not all cases need videos. Some can be explained with just images.
Current Case:
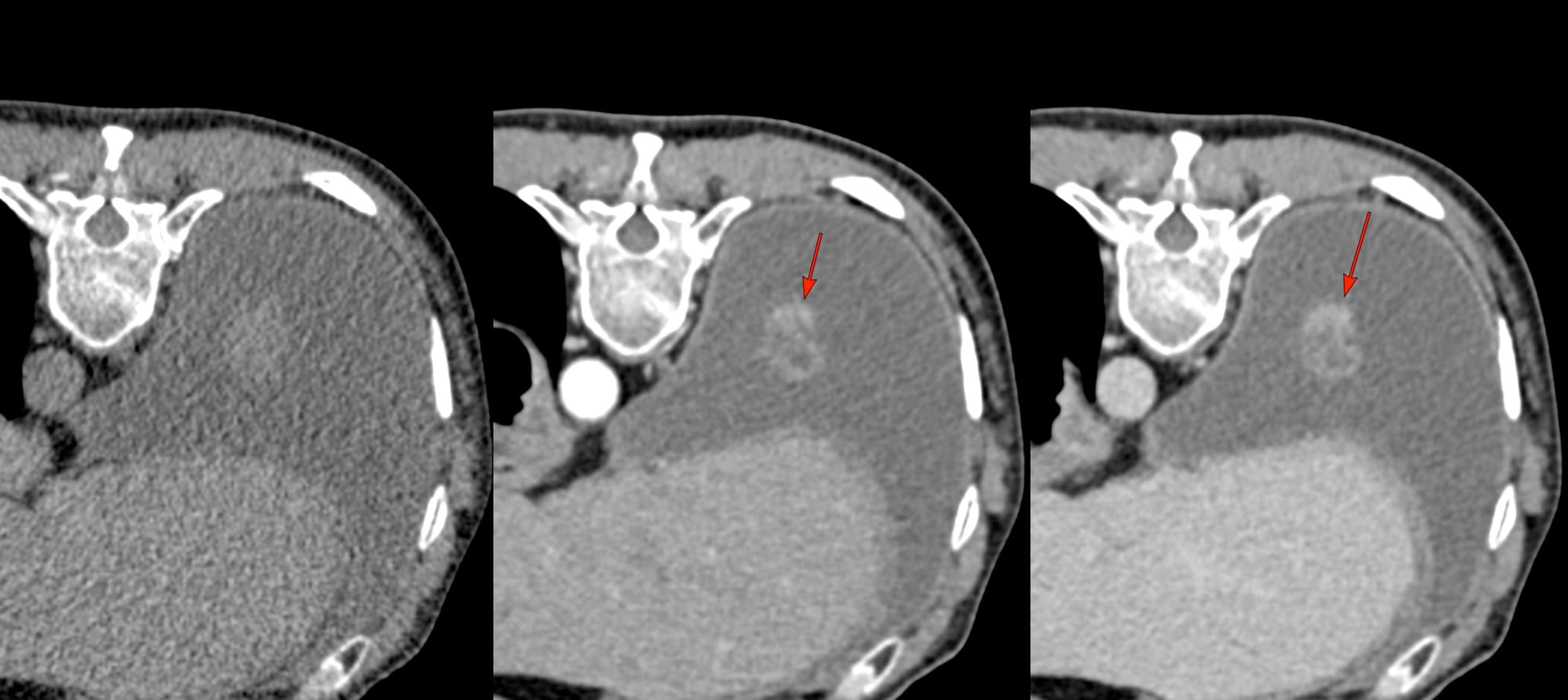
63-years old man had fever. X-ray and CT chest showed a pleural effusion.
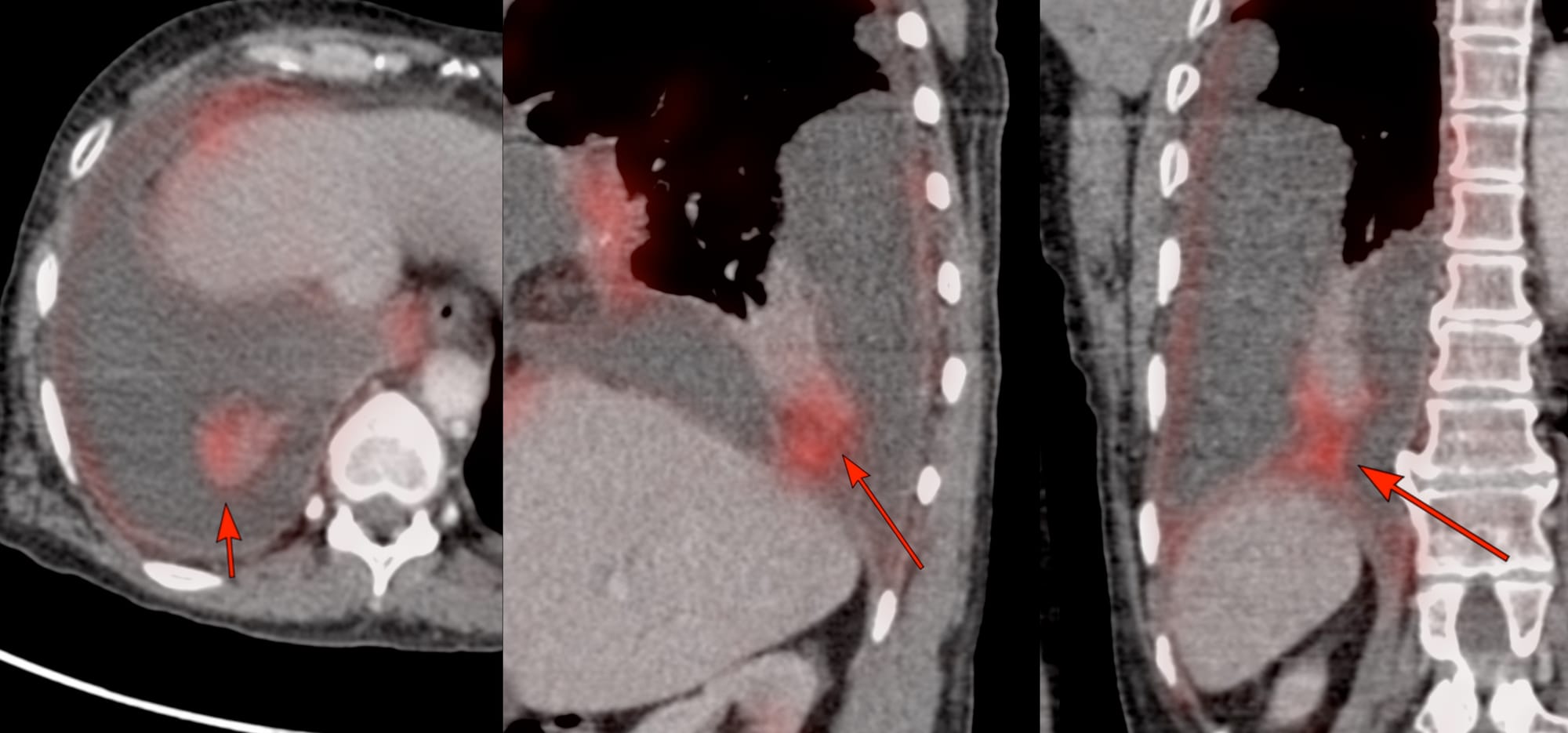
PET/CT showed a focal lesion arising from the posterior basal segment of the right lower lobe attached to the visceral pleura (arrows in Fig 1).
The patient was referred for a CT guided biopsy.
In the prone position, the effusion remained and the lesion was not well seen, so a contrast study was performed, which showed the lesion well (arrows in Fig 2).
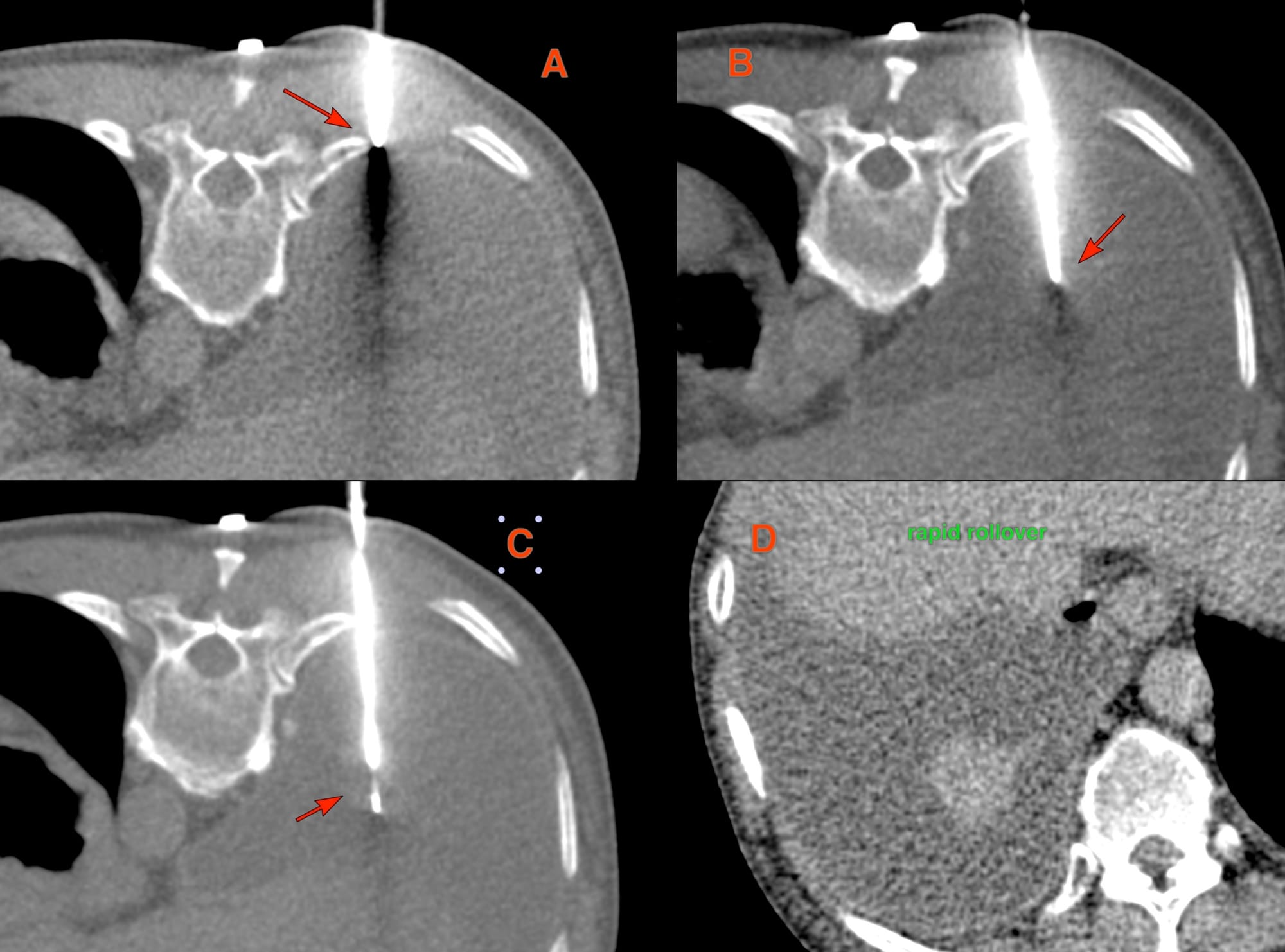
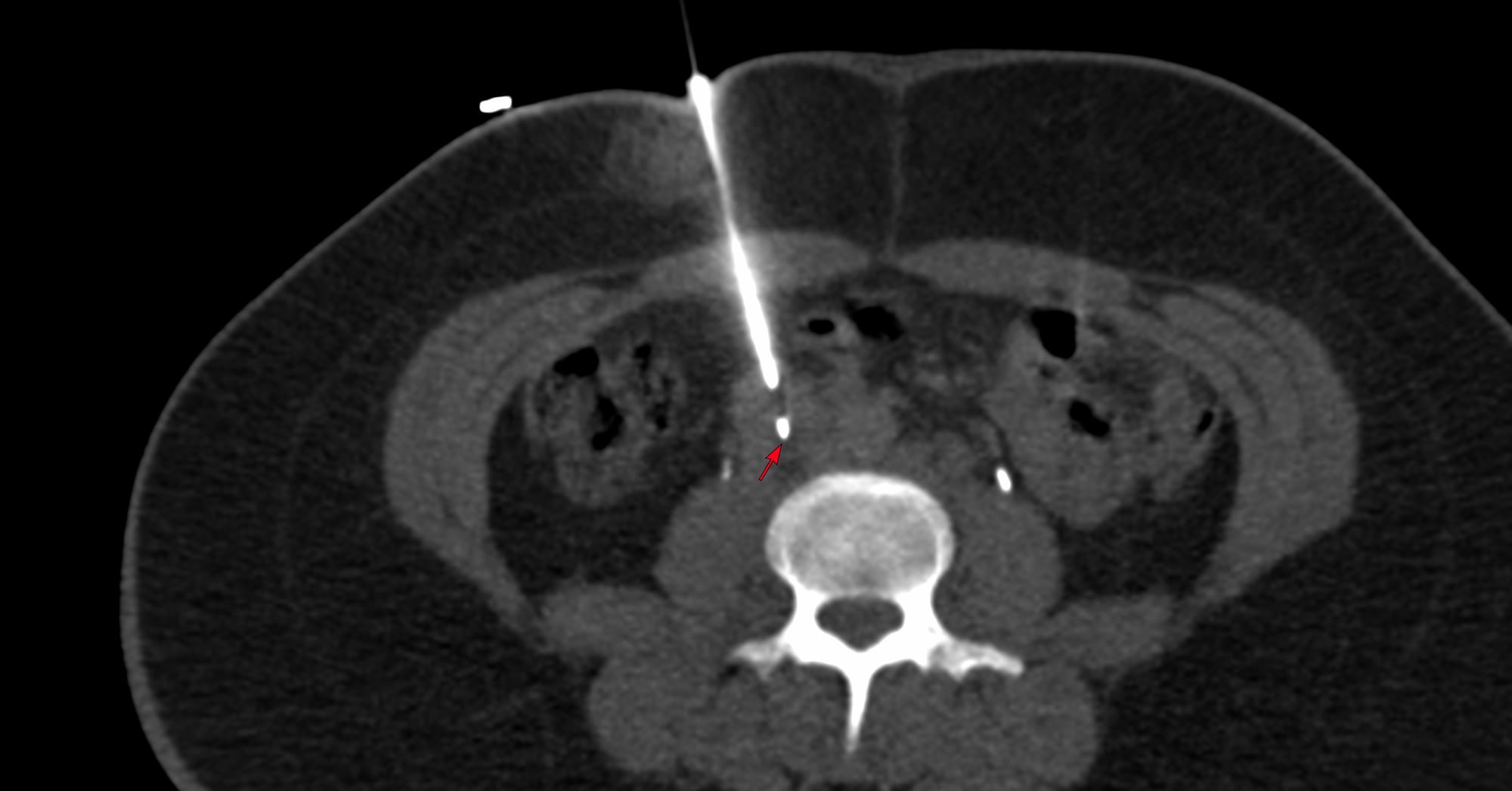
An 18G Cook coaxial biopsy gun (Fig. 3) was introduced into the lesion through the parietal pleura (arrow in A), and then through the effusion into the lesion (arrow in B). The gun was deployed (10 mm throw) (arrow in C) and 5 cores were obtained for histopath and 3 for microbiology. After 8 minutes, the needle was withdrawn.
The final diagnosis was GeneXpert negative, but histopath and culture positive tuberculosis.
There is some resistance to performing lung biopsies in the presence of pleural effusions and pneumothoraces, which is unfounded. There is no need to tap a patient dry...you can just go through the pleural disease and biopsy the lung.
Region: Chest
Age: 63 years
Findings: Exophytic nodule from lung - lower lobe
Lesion Biopsied: Same lesion
Size of Lesion: 23.8 mm z axis x 18.3 mm - avg - 21.0 mm
Gun: 18G Cook, 10 mm throw, long
No of cores: 5 for histopath and 3 for micro
Sedation: No
Position & Approach: Prone, transpleural effusion
Time Taken (marker to wash-out): 8 mins
Complication: None
Level of Difficulty: 3/5
Diagnosis: Tuberculosis
Previous case of a transpleural subcarinal node biopsy.

Table of Contents - Other Transpleural Biopsies
Previous Posts:
Other Sites and Cases:
Case of the Day on YouTube
{kind=link}