Index and Table of Contents
174 Cases with Videos
4 Cases with Images
2 Snippets
5 Lectures
4 Cases of the Day (CODs)
Table of Contents
Table of Contents
New Onetime Lifetime Subscription
Payment
To make the site more accessible, we have decided to remove the yearly subscription and keep only a one-time, lifetime payment to get access to all content at www.ctchestreview.com and www.ctbiopsy.com. These sites are linked and hence one payment gives access to both sites, but the
 Bhavin Jankharia
Bhavin Jankharia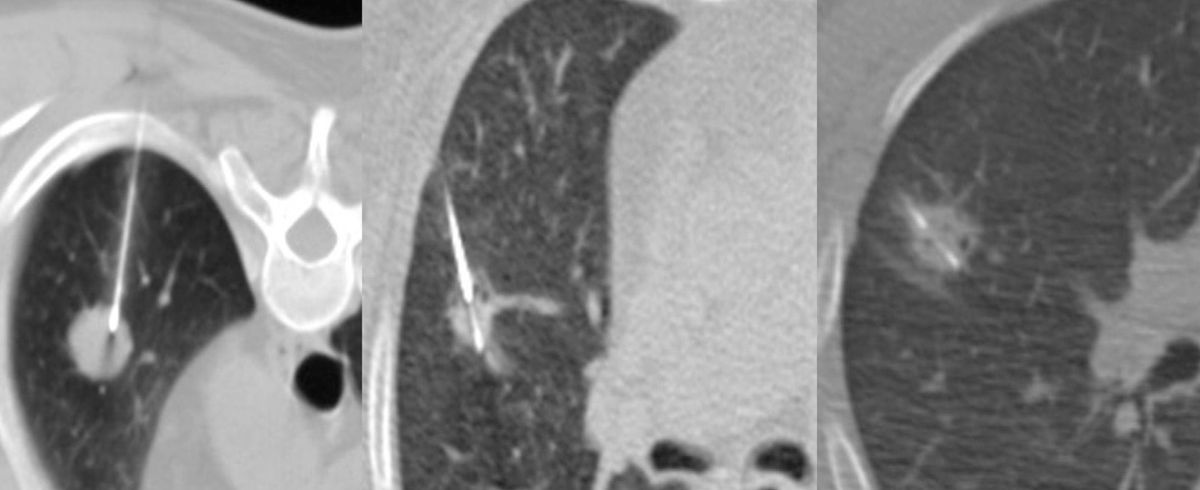
Not all cases need videos. Some can be explained with just images.
Current Case:
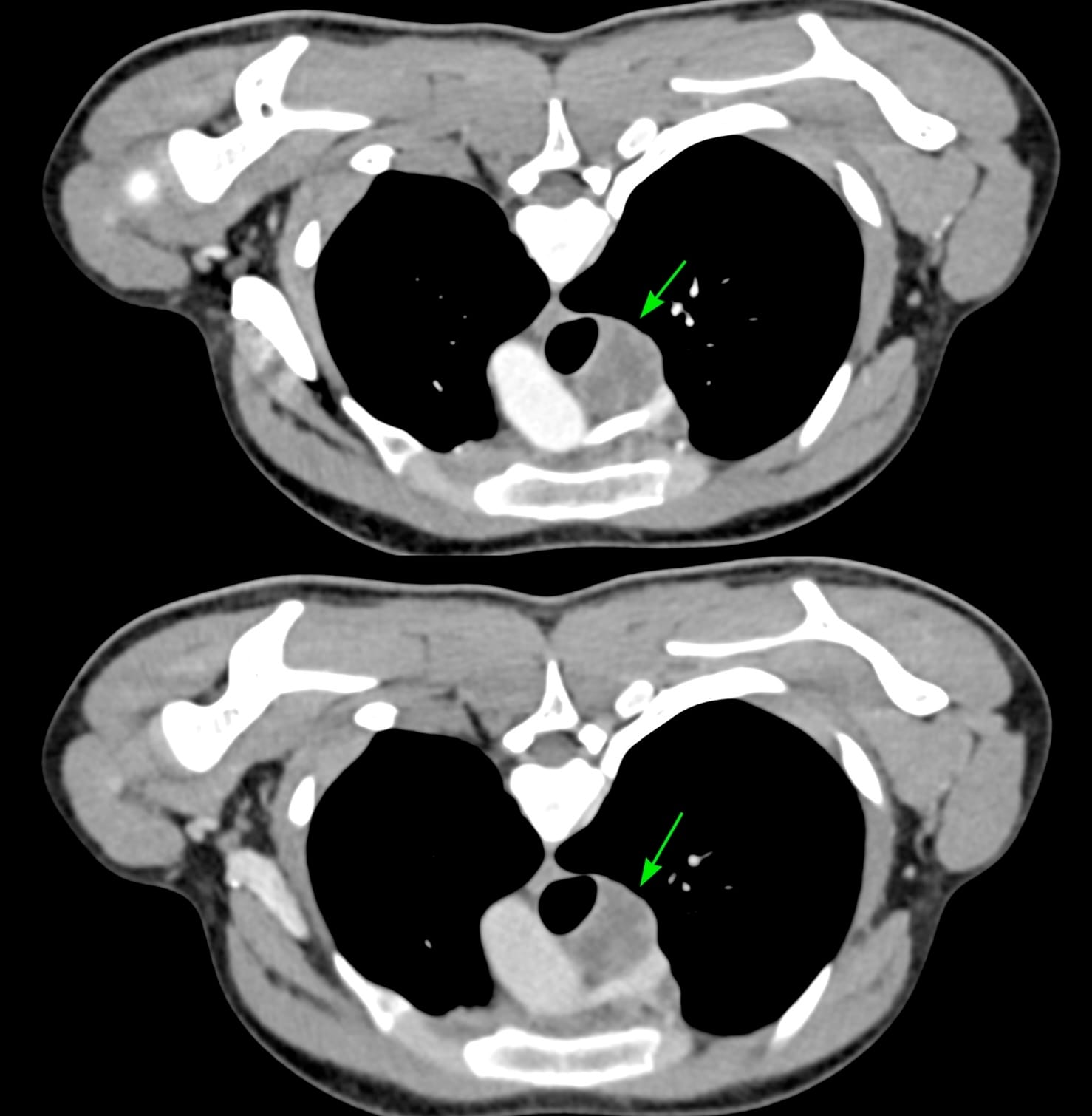
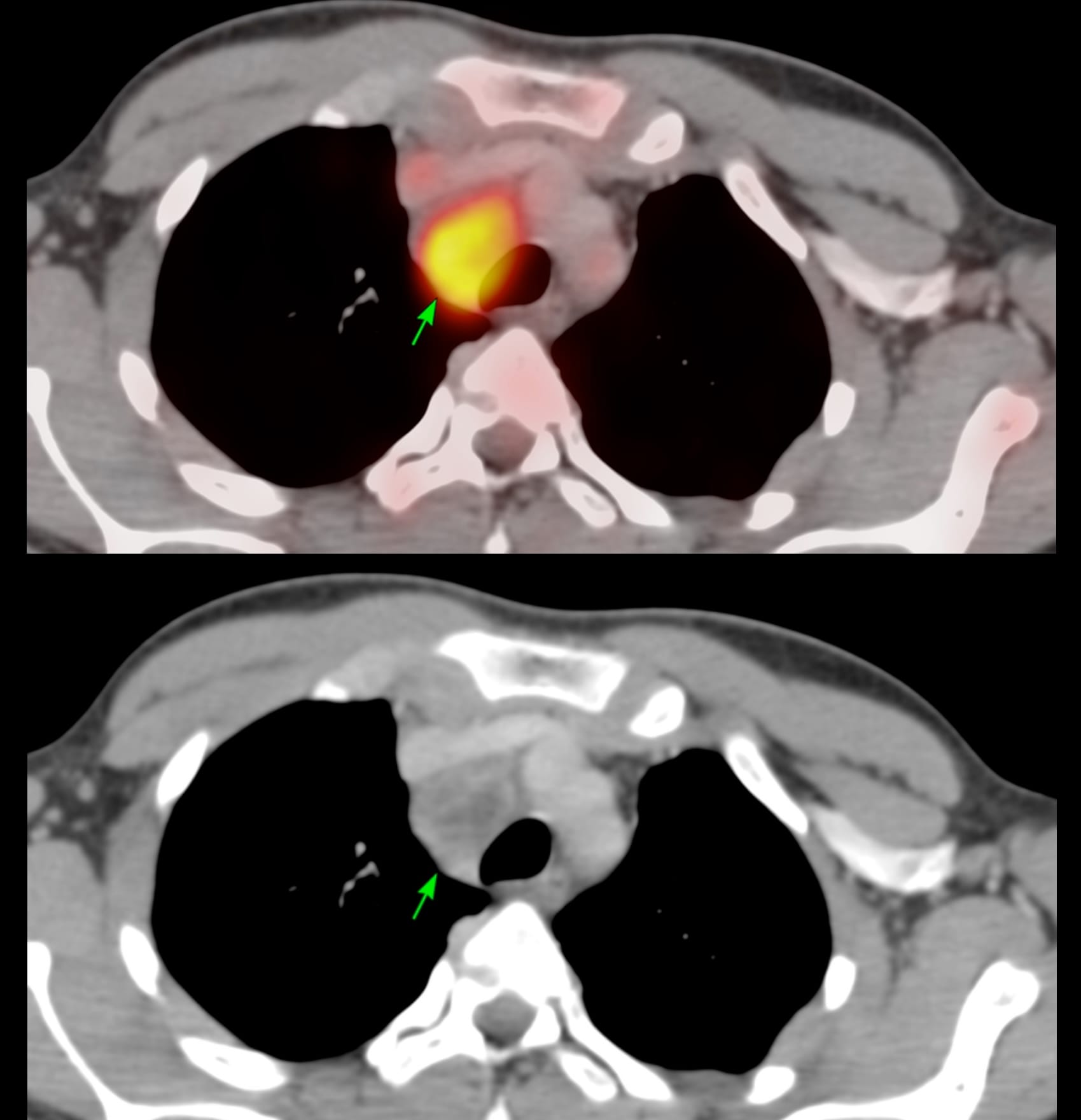
17-years old with fever had a PET/CT that showed a necrotic right paratracheal node - 4R - and was referred for a CT guided biopsy.
The patient was referred for a CT guided biopsy.
Pulmonologists here will jump saying this can be easily done with EBUS, but I have been doing these biopsies under CT guidance since 1995 - over 31 years now, and there is no reason to give them up. EBUS is non-inferior to CT, not better...and it is cheaper, faster, easier and simpler.
Arterial and venous phase studies in the prone position just prior to the biopsy showed the necrotic node well.