
New Onetime Lifetime Subscription
 Bhavin Jankharia
Bhavin Jankharia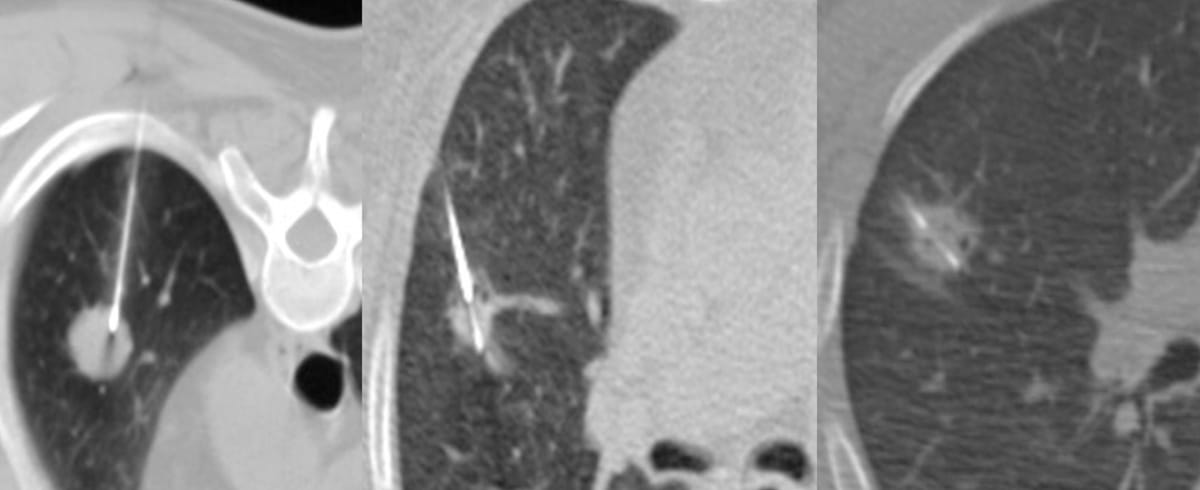
Not all cases need videos. Some can be explained with just images.
Current Case:
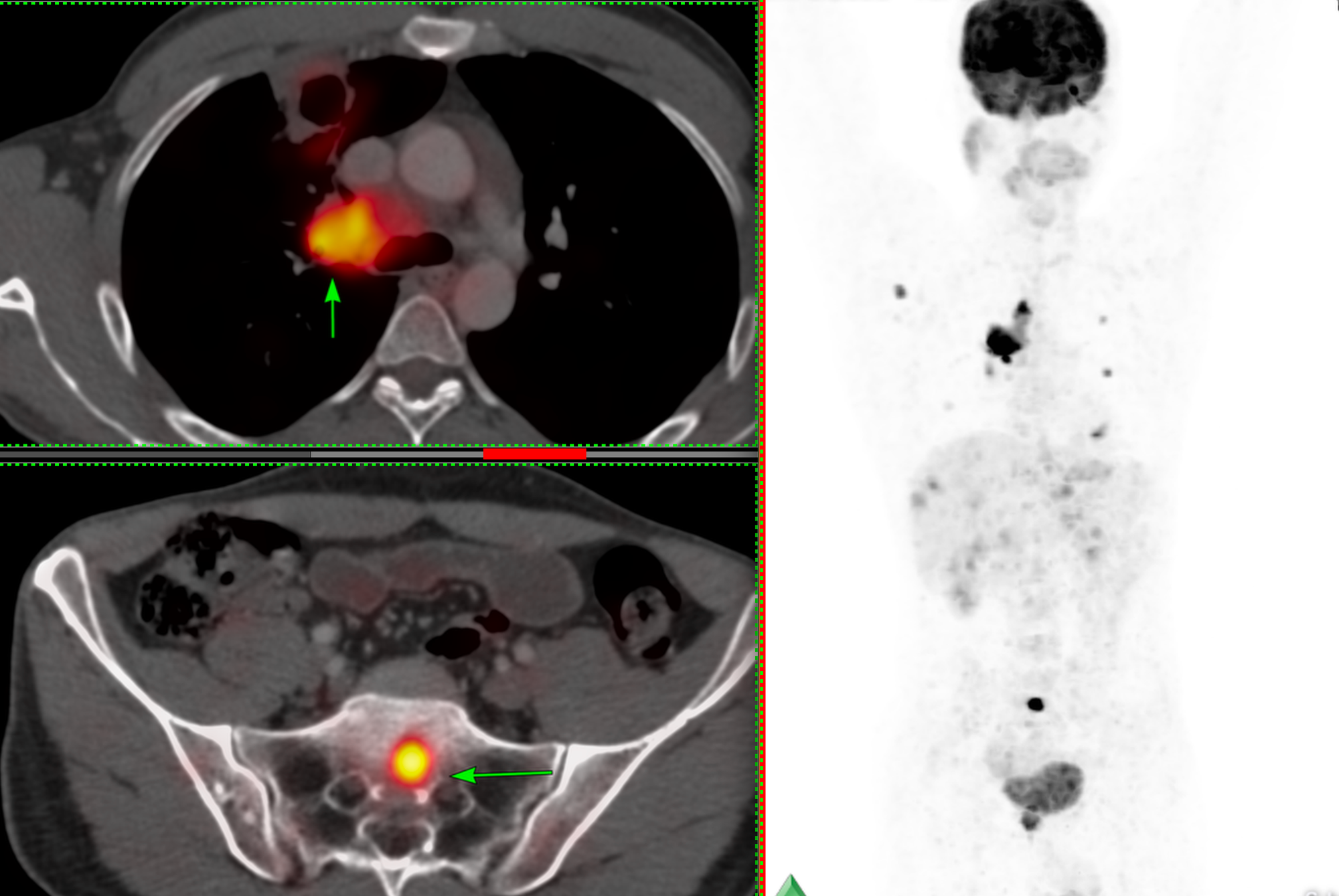
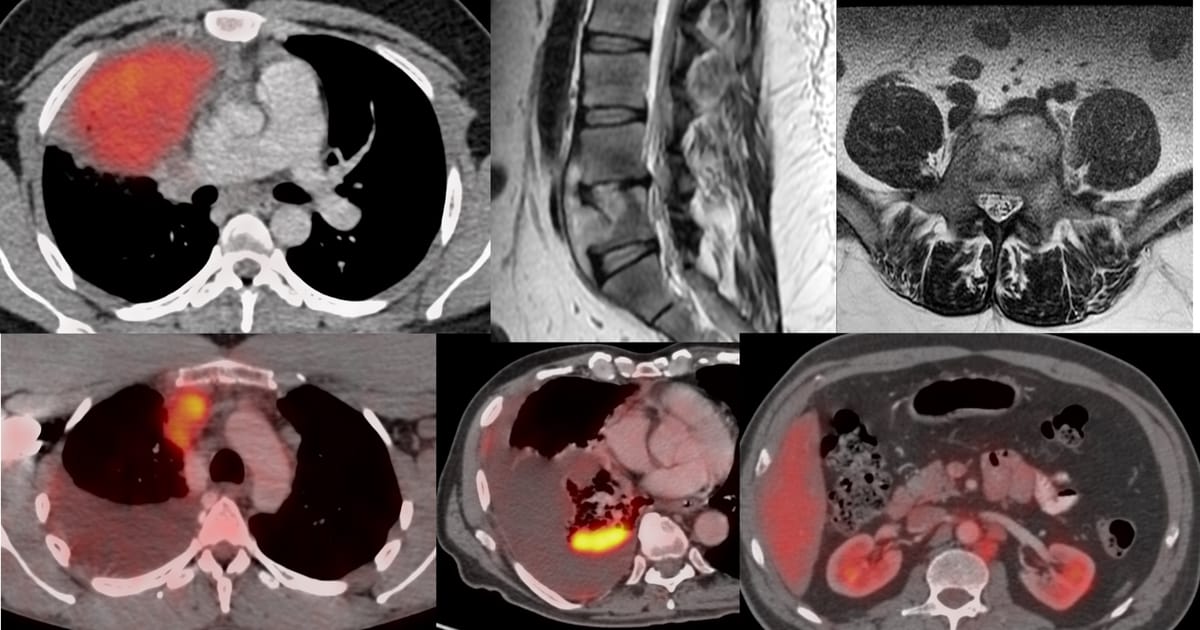
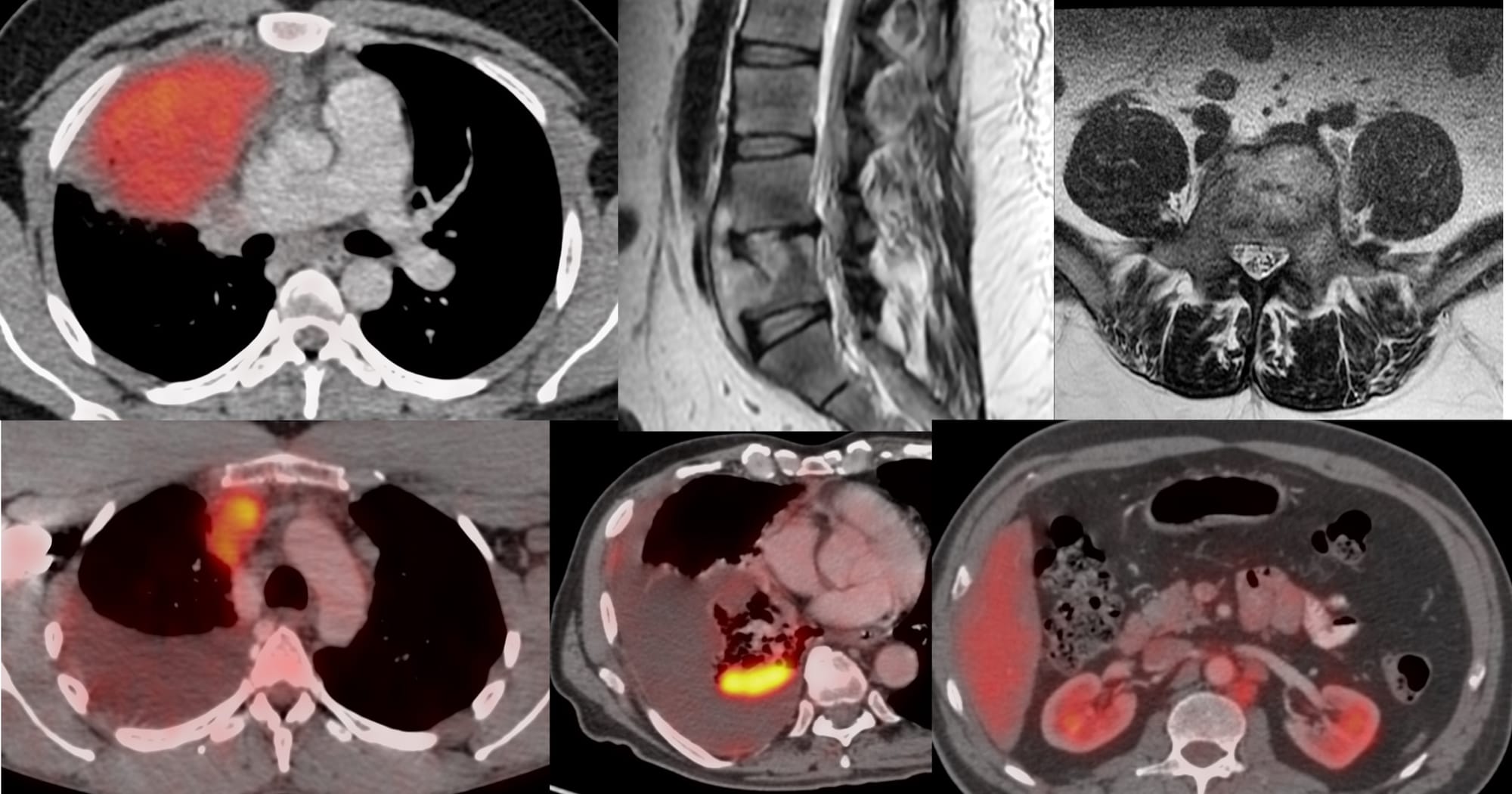
43-years old treated buccal ca had progressive lung and nodal lesions (arrow in to panel), stable liver lesions and a new S1 osteolytic lesion on PET (arrow in bottom panel) (Fig. 1).
The patient was referred for a CT guided biopsy of the sacral lesion.
Fig. 2 shows how the lesion could be approached in the the axial plane by charting a route from the posterior margin of S1 on the right, through the S1/S2 disc into the lesion, between the S1/S2 sacral foramina and the central canal, without injuring the nerves.
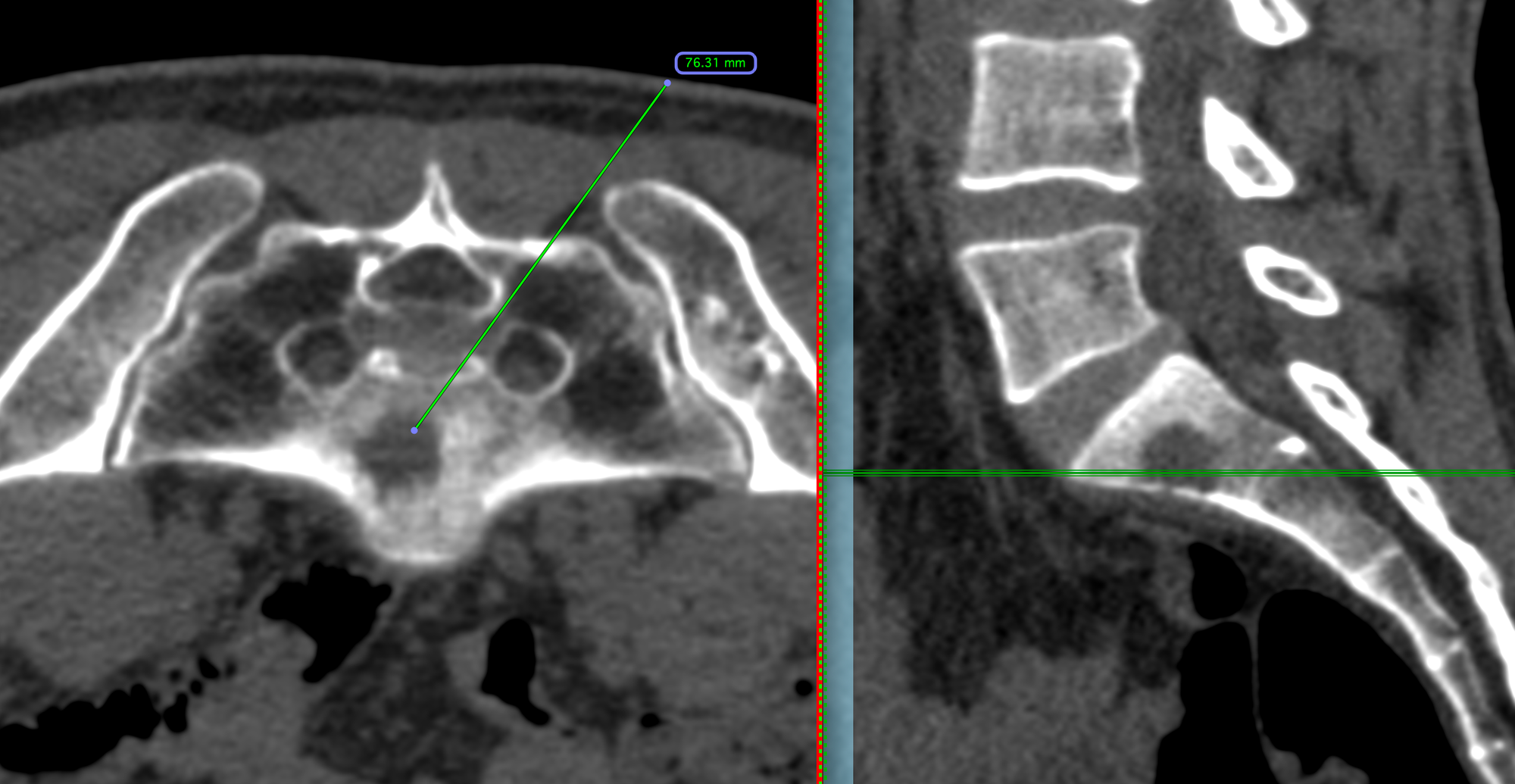
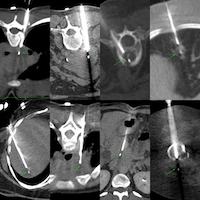
Fig. 3 shows the biopsy. The 11G bone biopsy needle at the edge of S2 (arrow in A) and then with a hammer tapped between the central canal and S1/S2 foramen (arrow in B) through the thin sliver of bone and then past it (arrow in C) and then into the osteolytic lesion. An 18G BARD, 20 mm throw gun was deployed and 7 cores were obtained for histopath and 1 for PDL1 in 9 minutes.
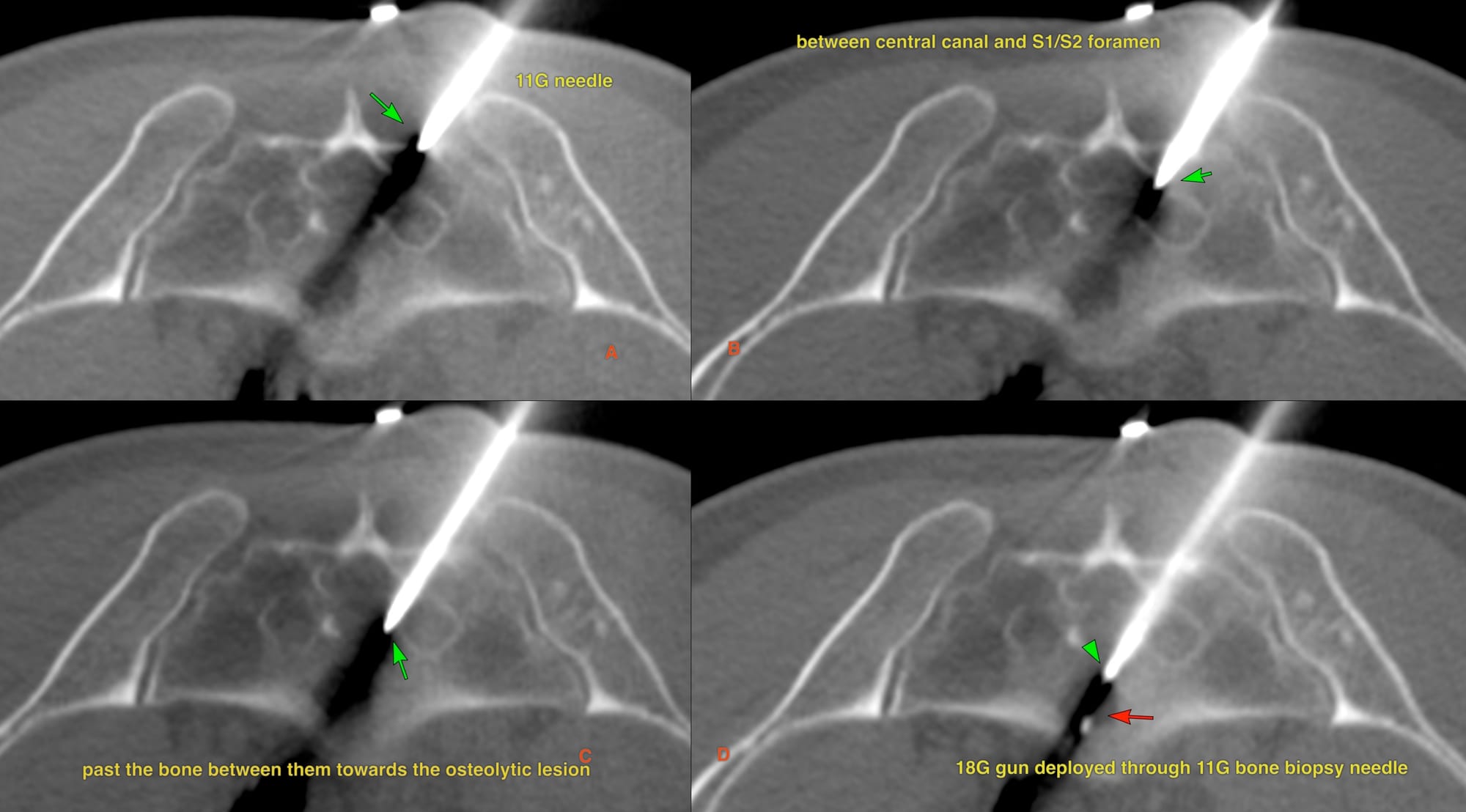
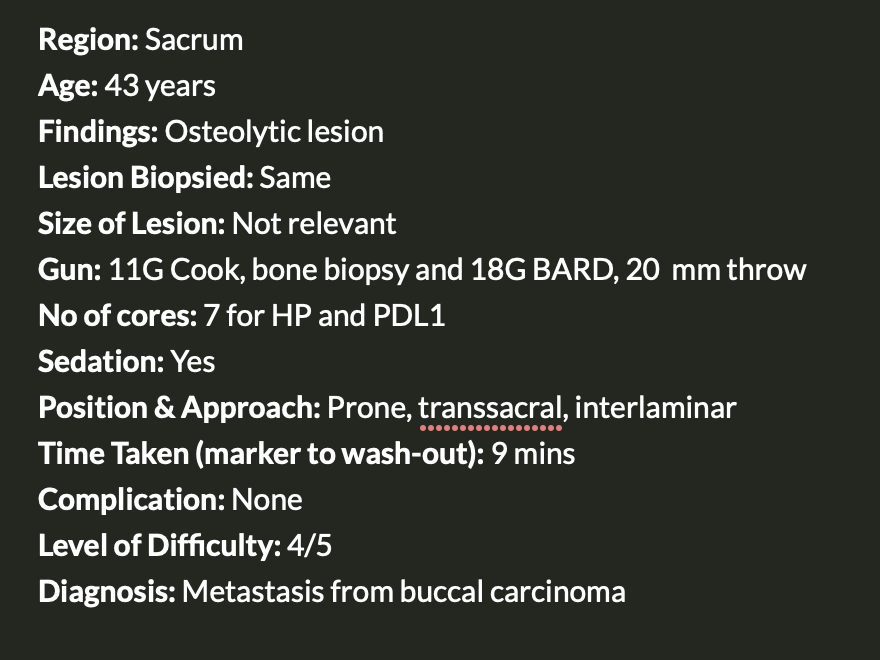
Fig. 4 shows the summary slide - the final diagnosis was metastasis from buccal carcinoma.
A similar biopsy was described as Case 166 here.
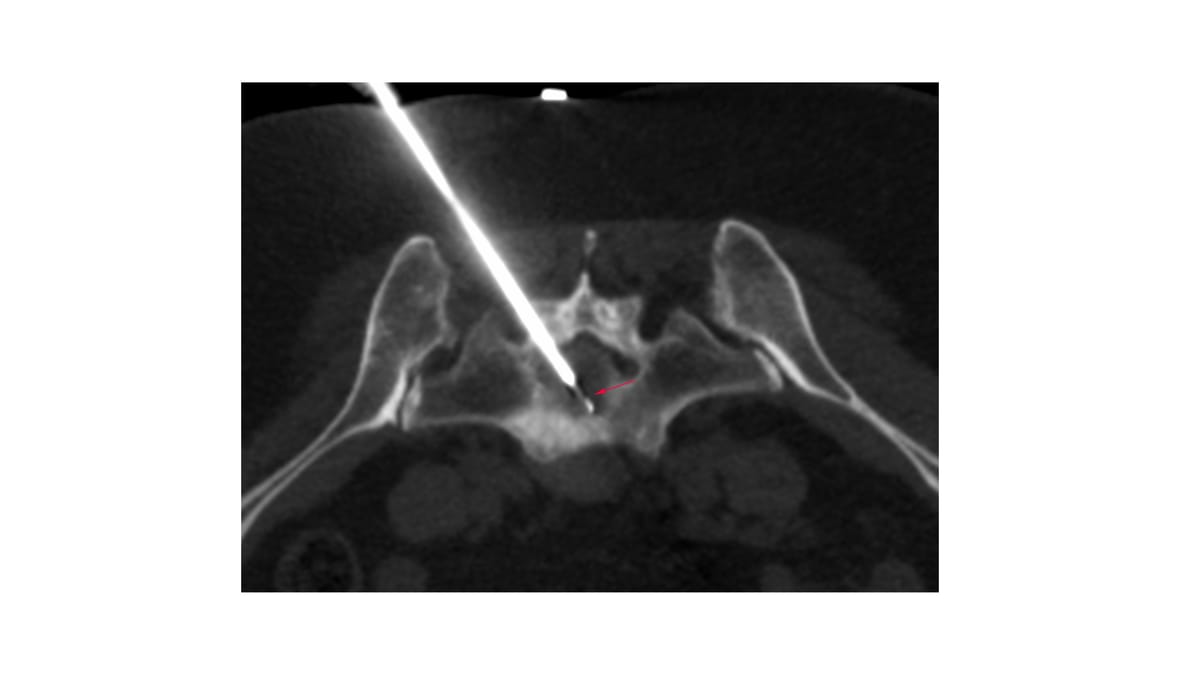
Table of Contents and Other Spine Biopsies
Bhavin Jankharia
Previous Posts:
Other Sites and Cases:
Case of the Day on YouTube
{kind=link}