
Index and Table of Contents
174 Cases with Videos
2 Cases with Images
2 Snippets
5 Lectures
4 Cases of the Day (CODs)
New Onetime Lifetime Subscription
 Bhavin Jankharia
Bhavin Jankharia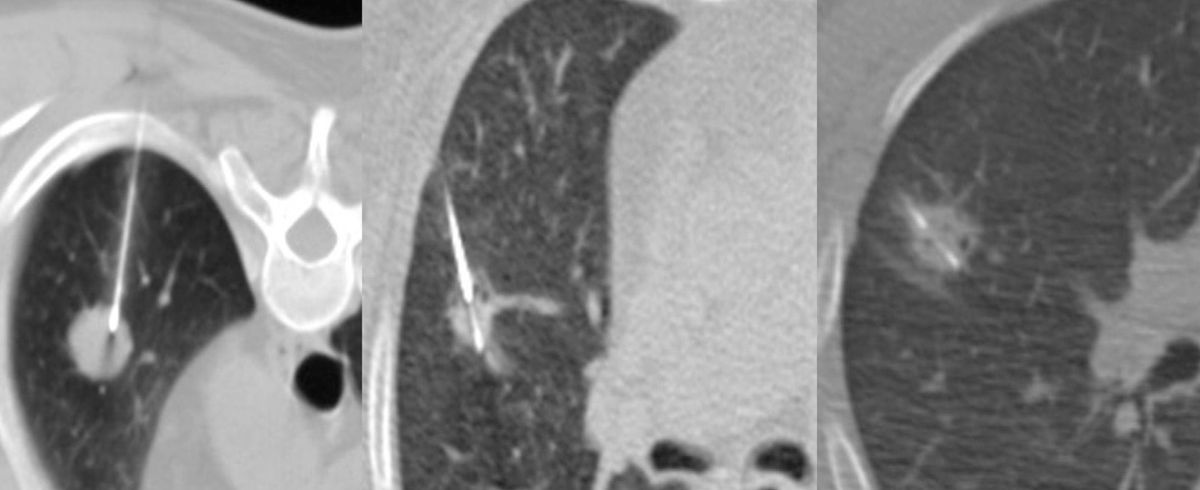
Not all cases need videos. Some can be explained with just images.
Current Case:
22-years old treated 5 years ago for dysgerminoma had back back and MRI showed a right iliac bone lesion. PET-CT (Fig. 1) showed uptake in the lesion (A) but also aortocaval (C) and retroperitoneal para-aortic nodes.
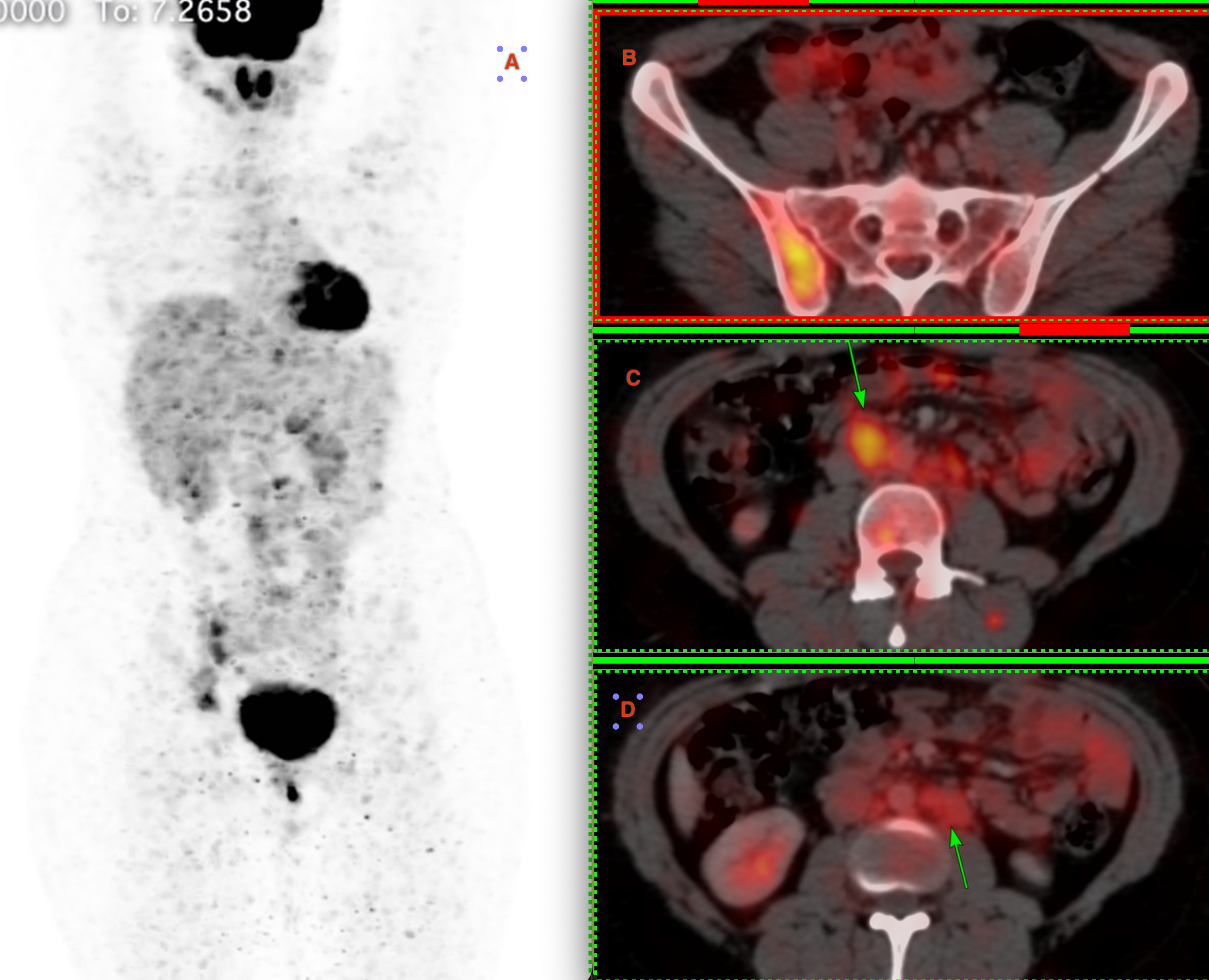
The aortocaval node had the most activity and the onco team asked for a biopsy of this node.
The patient was referred for a CT guided biopsy.
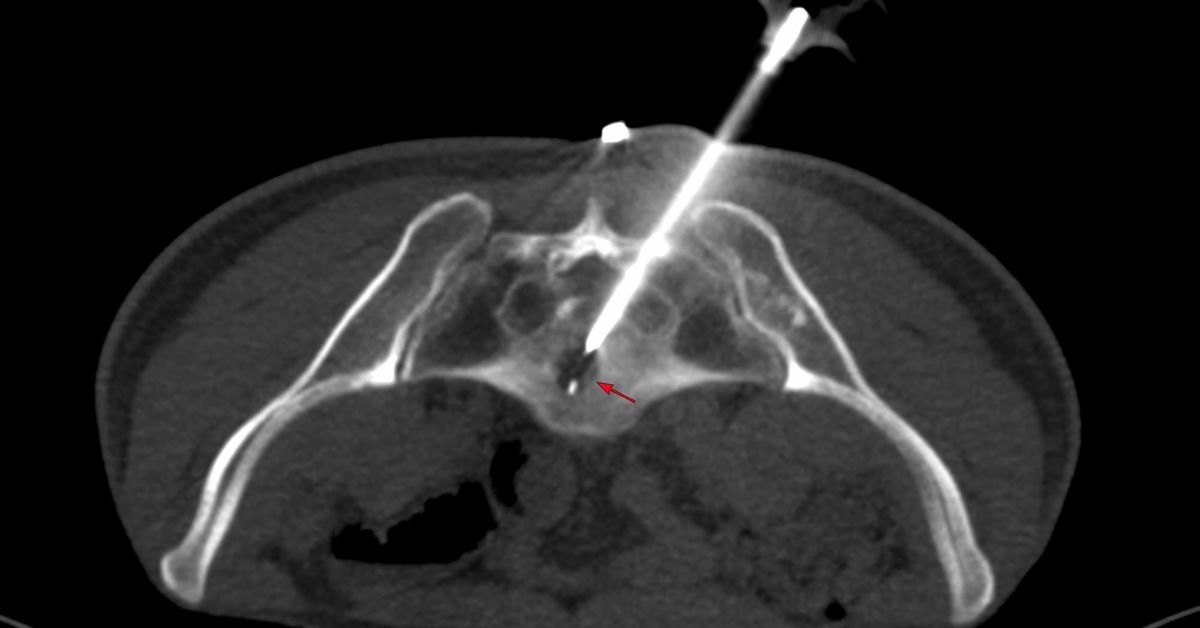
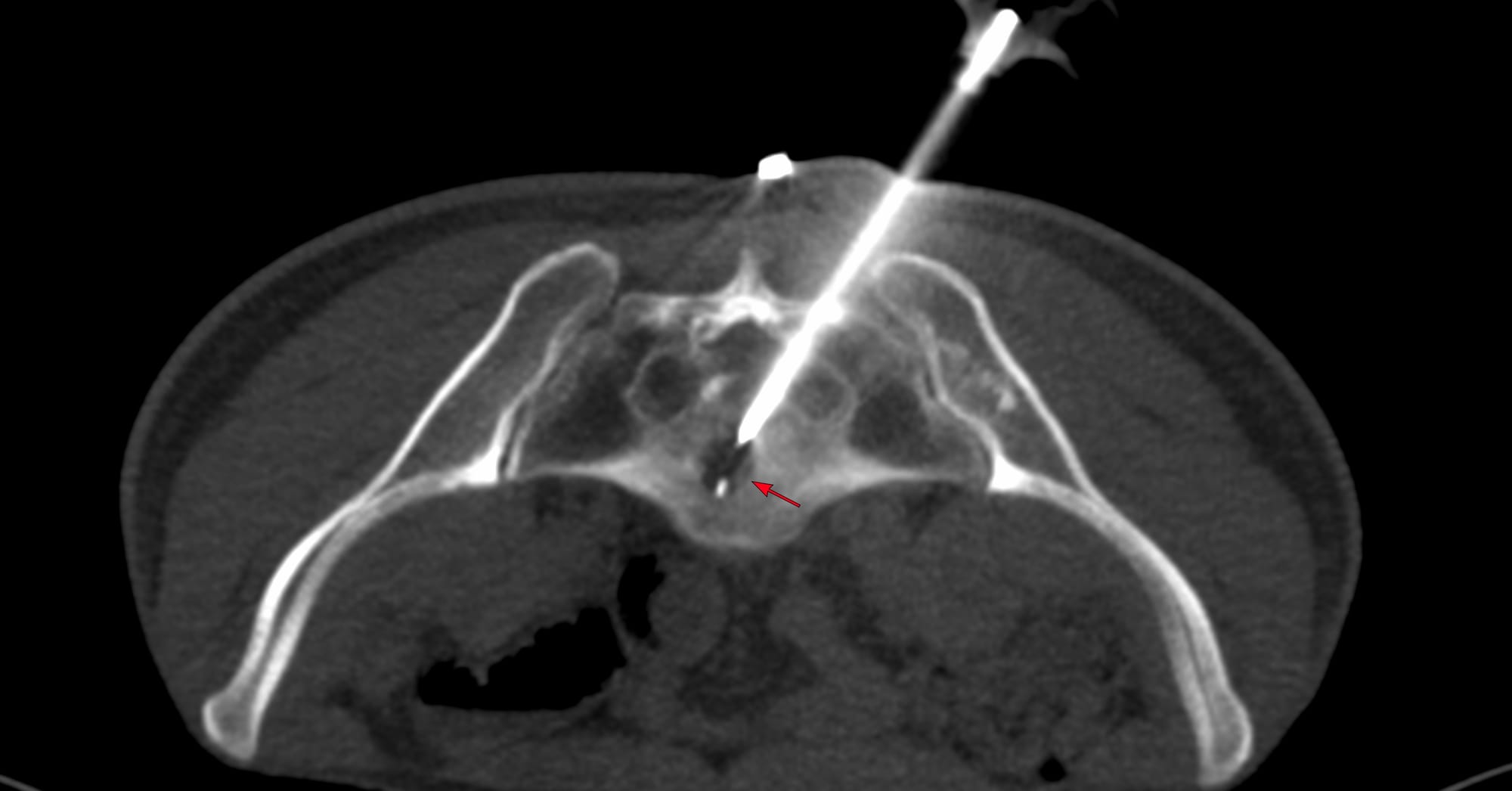
The only approach is anterior in this case (Fig. 2). A posterior approach, though possible in any instances, is difficult in her because of the anatomy, unless you go transvertebral.
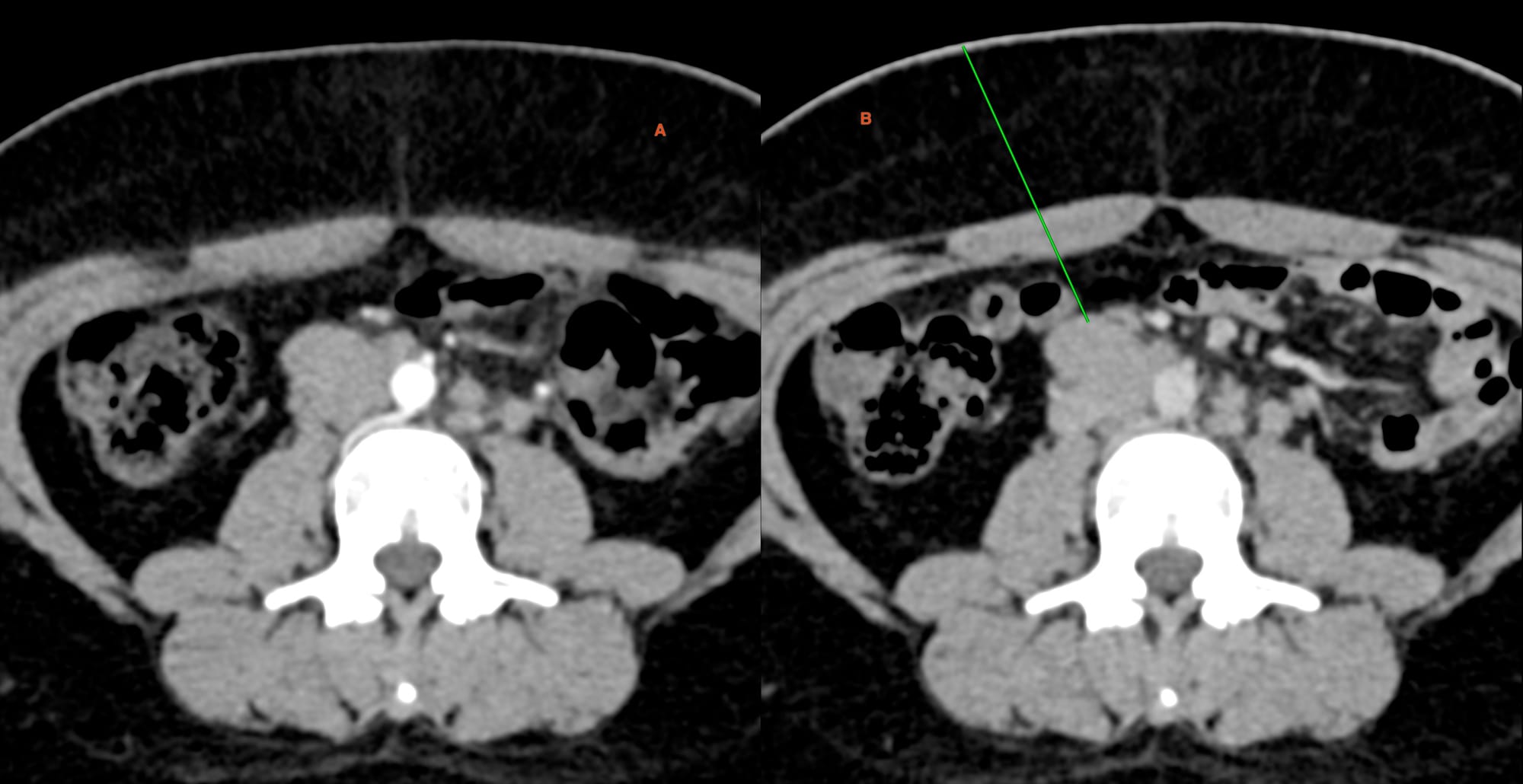
Fig. 3 shows the AP diameter. The posterior margin has a vein draining into the IVC, so care has to be taken not to overshoot.
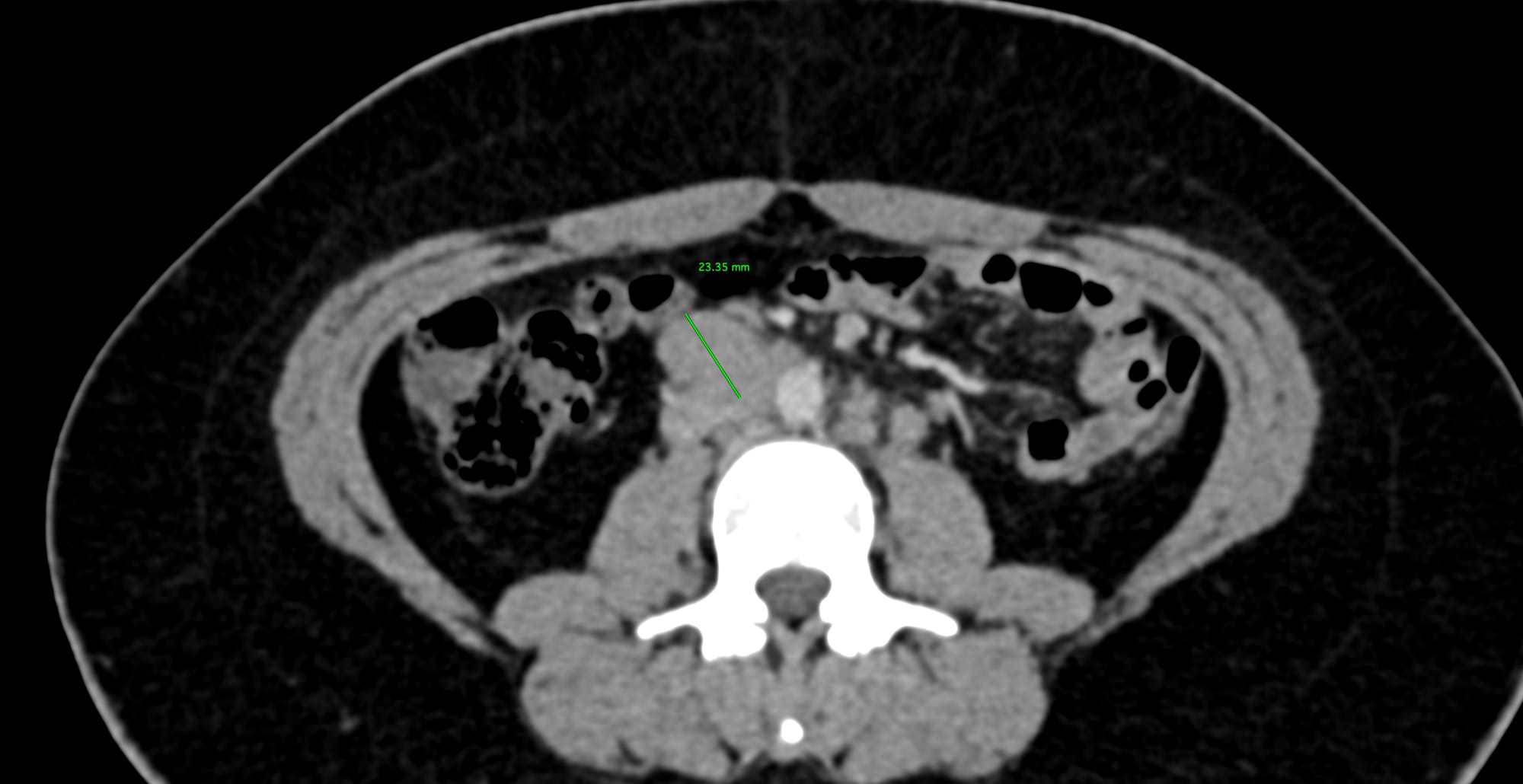
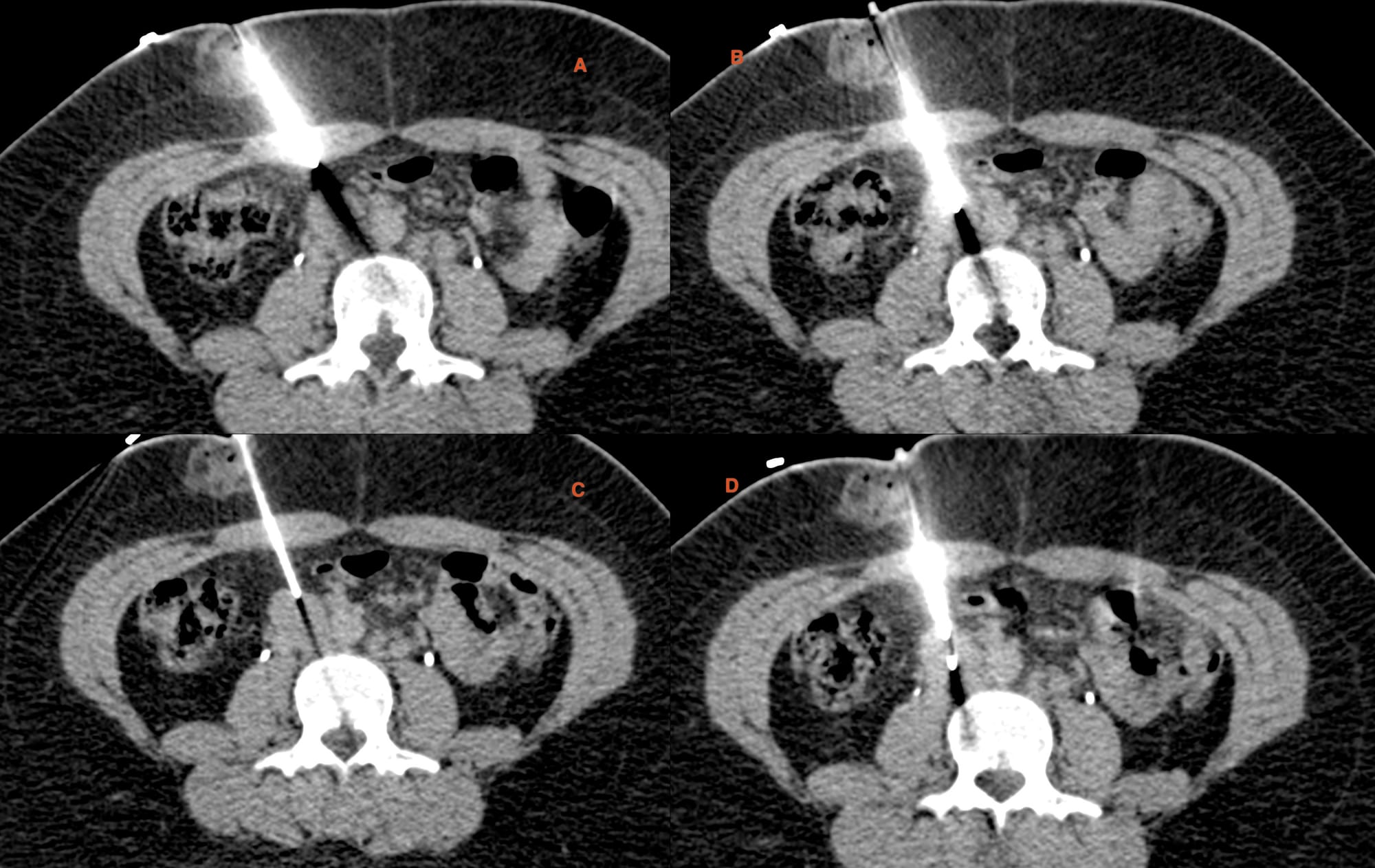
Fig. 4. Panel shows the 18G BARD, 20 mm throw gun with a straight entry into the node (A, B). After withdrawing the stylet, the canal is pulled up to the proximal edge of the node (C). I used a hub to reduce the throw to 10 mm (D) and deployed the gun.
As Fig. 5 shows, it took 9 minutes for 5 cores for histopath.
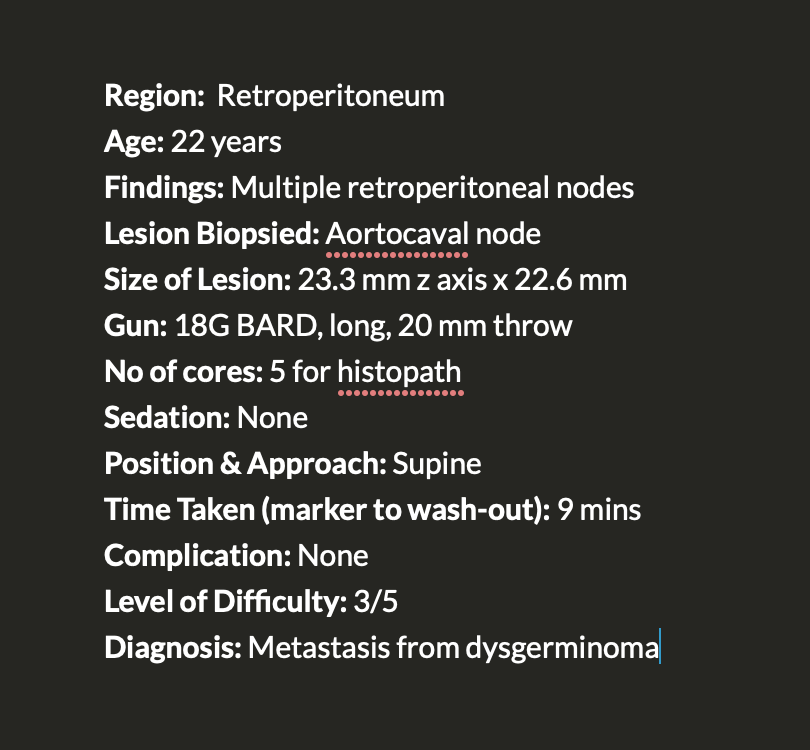
Diagnosis was metastasis from ovarian dysgerminoma.
A similar biopsy was described as Case 110 here.
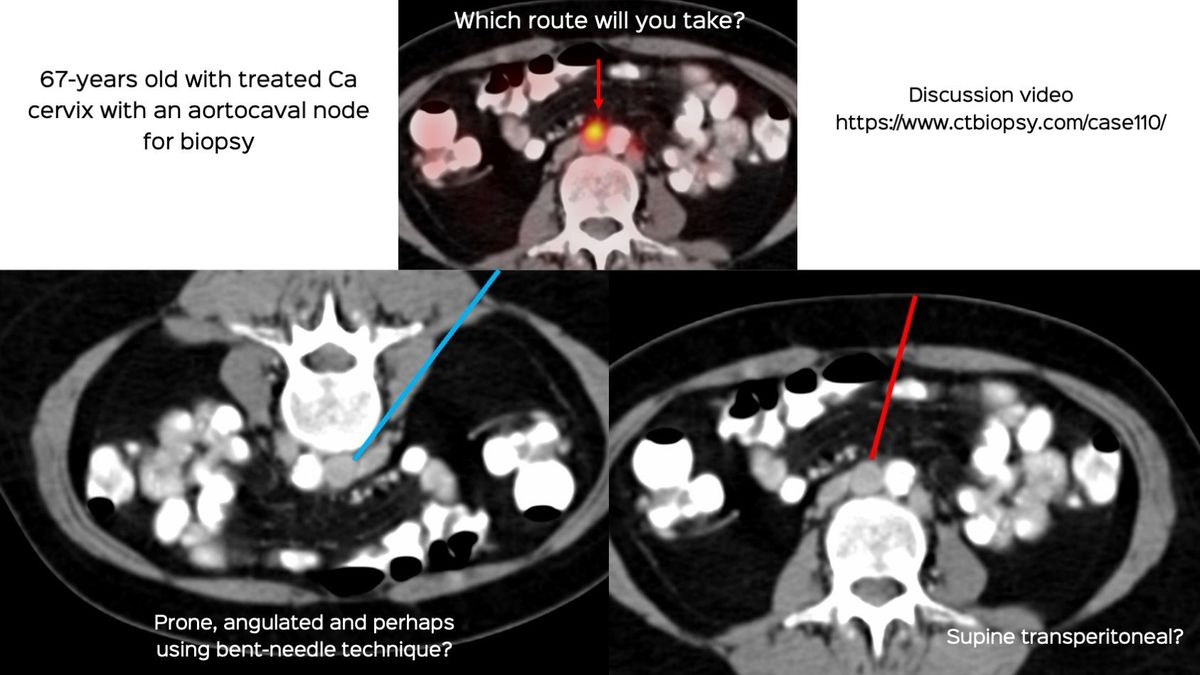
Table of Contents - Other Retroperitoneal Lesion Biopsies
Previous Posts:
Other Sites and Cases:
Case of the Day on YouTube
{kind=link}