Index and Table of Contents
174 Cases with Videos
5 Cases with Images
2 Snippets
5 Lectures
4 Cases of the Day (CODs)
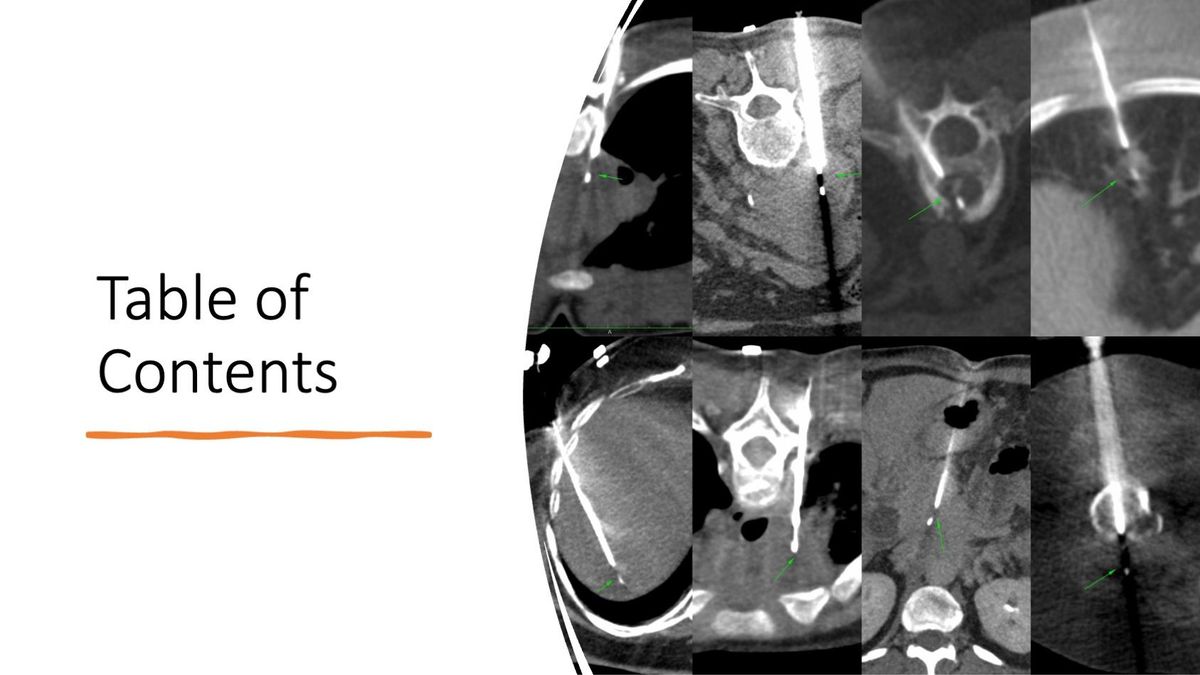
Table of Contents
Table of Contents
New Onetime Lifetime Subscription
Payment
To make the site more accessible, we have decided to remove the yearly subscription and keep only a one-time, lifetime payment to get access to all content at www.ctchestreview.com and www.ctbiopsy.com. These sites are linked and hence one payment gives access to both sites, but the
 Bhavin Jankharia
Bhavin Jankharia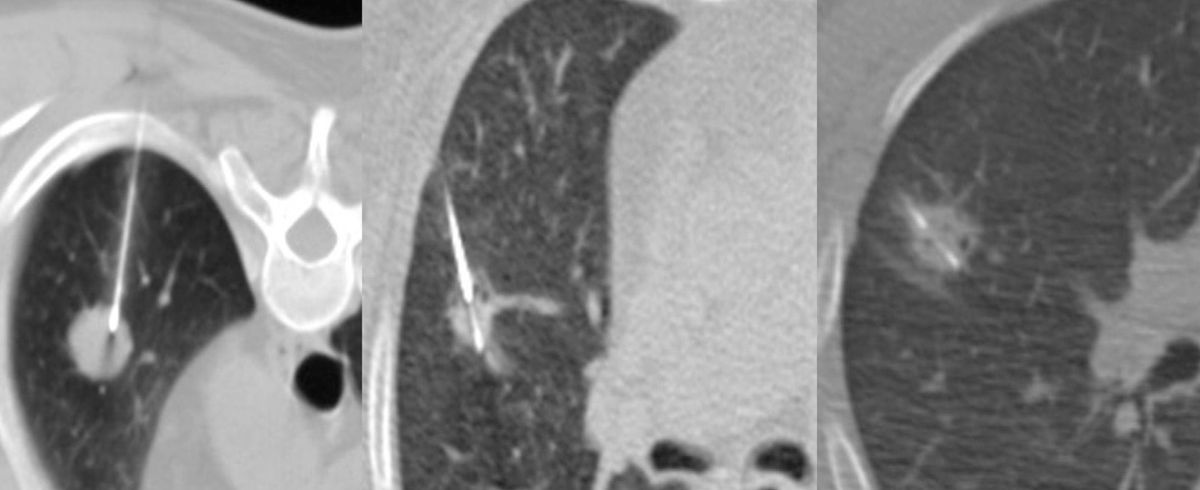
Not all cases need videos. Some can be explained with just images.
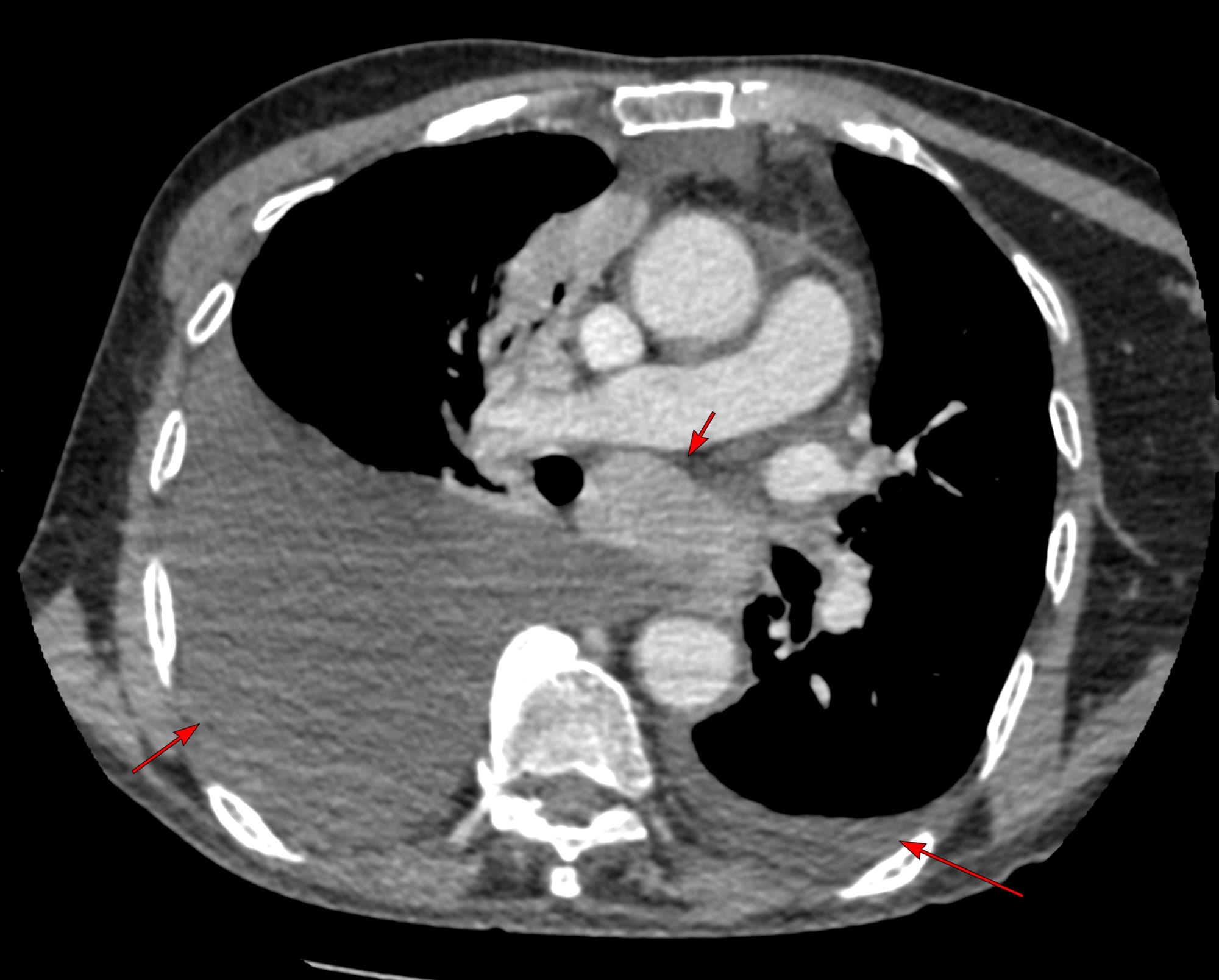
Current Case:
82-years old known to have T-cell non-Hodgkin's lymphoma had a PET in Jan that showed enlarged mediastinal and left supraclavicular nodes.
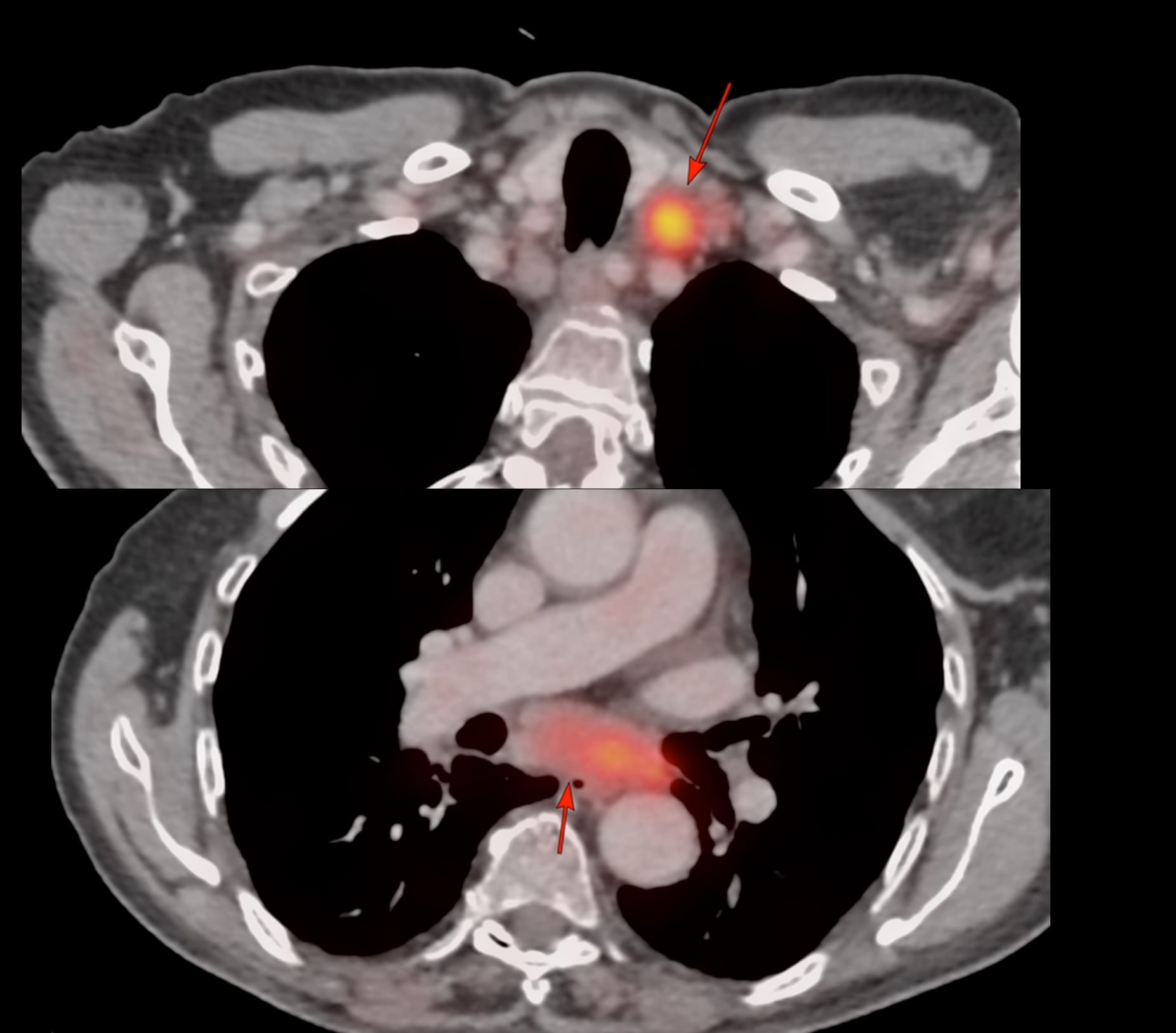
USG guided left supraclavicular node biopsy was negative for any specific diagnosis.
3 months later, he clinically worsened and CT scan showed the same nodes with mild increase in the subcarinal node size and bilateral effusions and he was referred for a CT guided biopsy of the subcarinal node. The short axis of the node was 25 mm, so biopsy was feasible.