
Not all cases need videos. Some can be explained with just images.
Current Case:
A 56-year-old man with carcinoma prostate had a PSMA PET (showing uptake in the prostate (A) and in the left 4th rib anteriorly (arrows in coronal MIP and B).
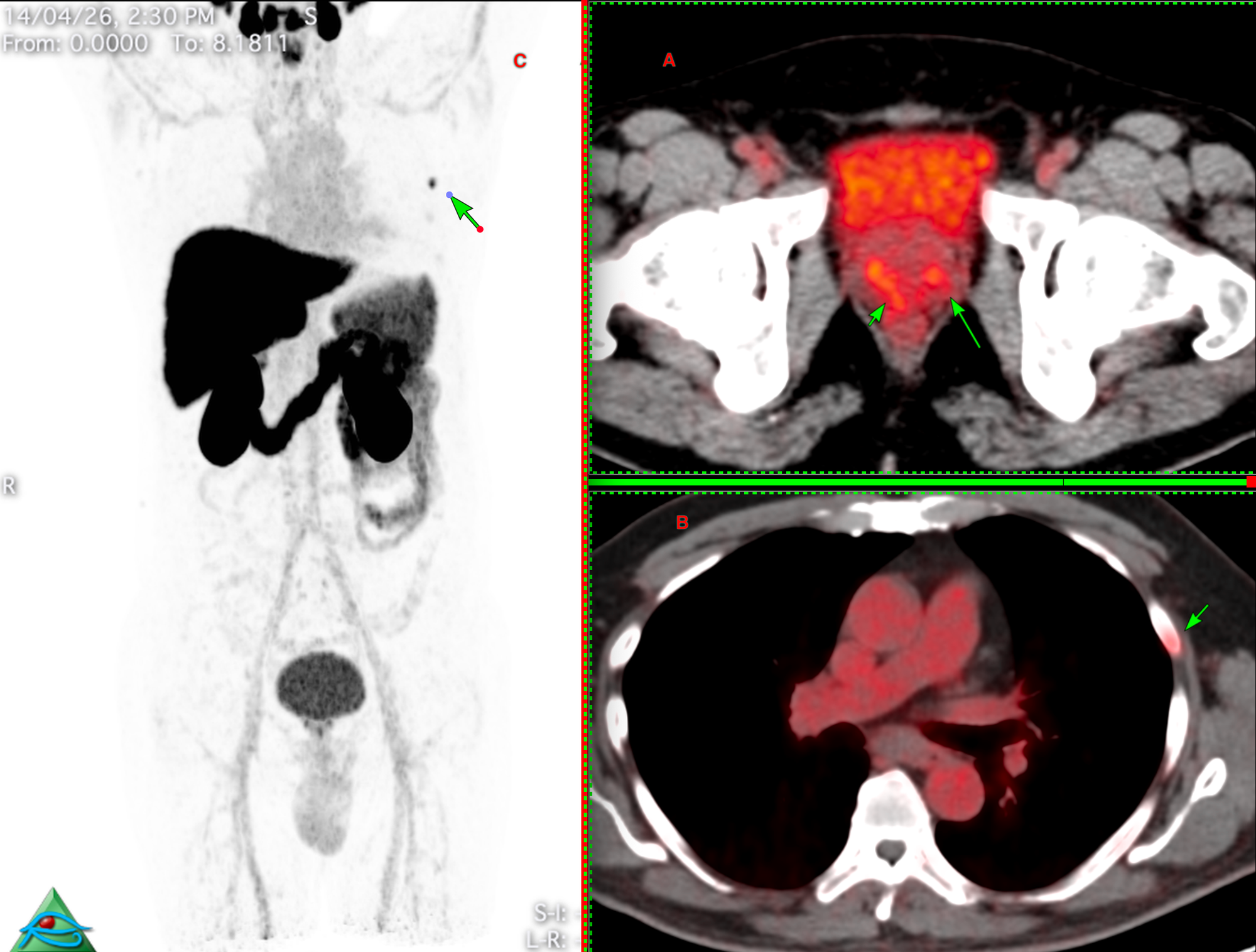
He was sent for an opinion on the rib lesion. In Case 60 at bstneoplasms.com, I discussed a similar case. Most such PSMA-avid rib lesions are benign and incidental — in a recent series by Ou et al. (Skeletal Radiology, 2025), only 5 of 19 biopsied PSMA-avid rib lesions (26%) were metastatic, compared with 82% for spine and 72% for pelvic biopsies.
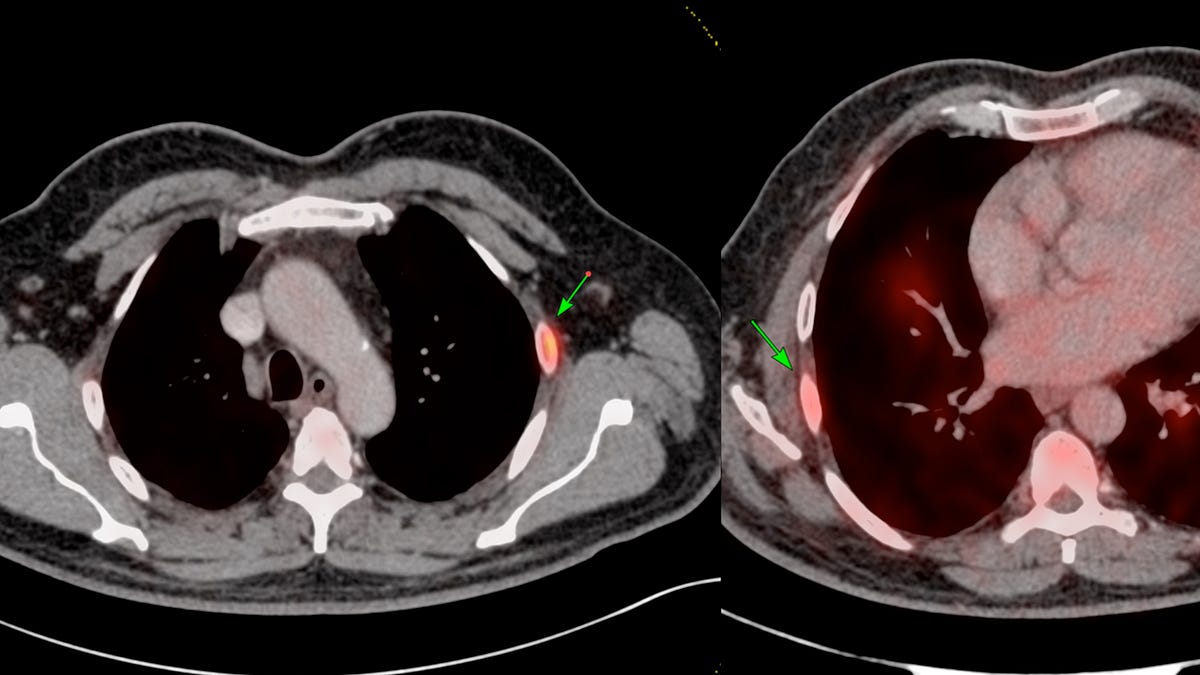
On the bone window and curved MPR images, the lesion had a sclerotic rim without cortical break and no extra-osseous soft tissue — features that favour a benign cyst or fibrous dysplasia. There was no chondroid matrix to suggest enchondroma.
The referring team still wanted tissue.