
Current Case:
A 72-year-old woman presented with neck pain.
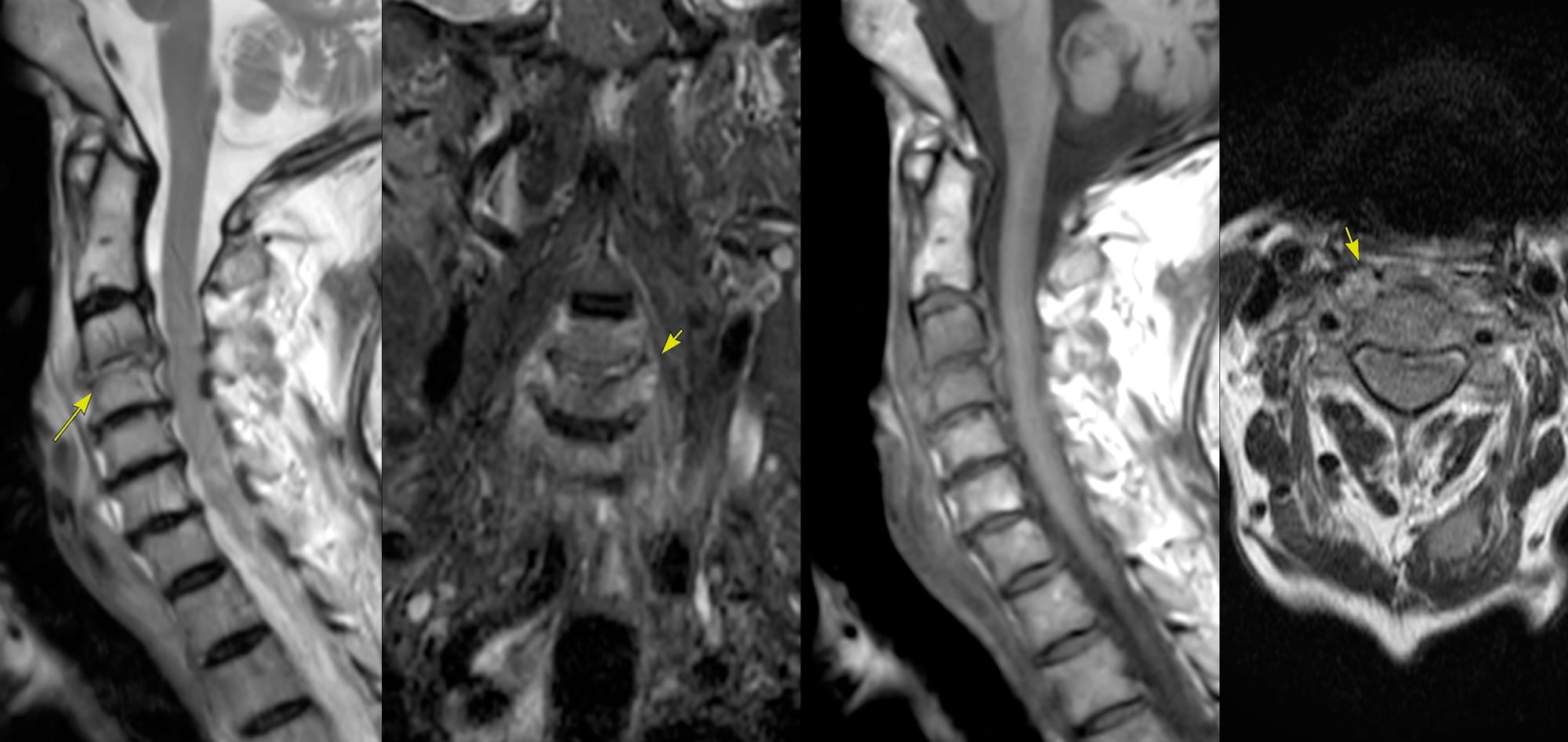
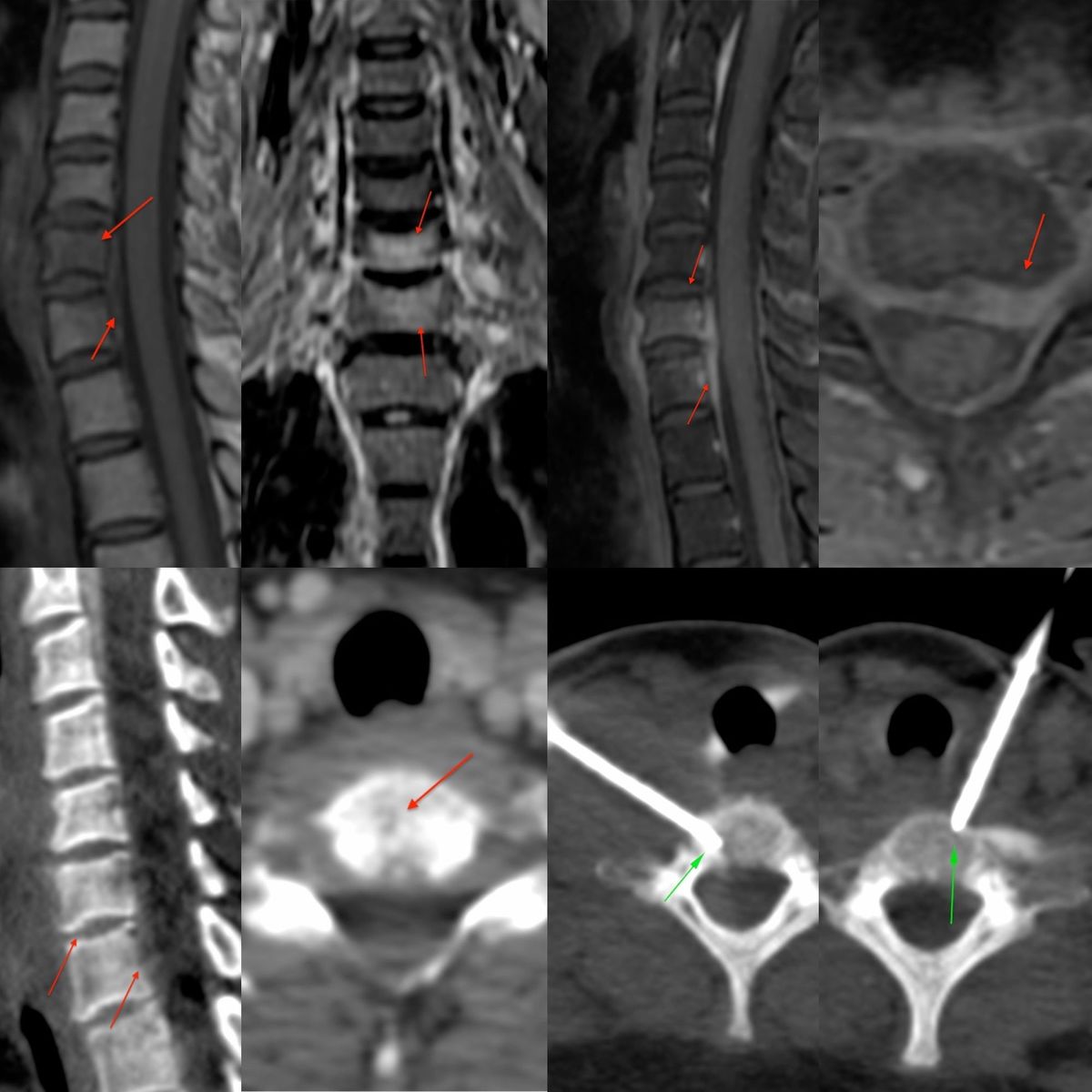
MRI (Fig. 1) showed a T2 bright C3-C4 disc with marrow edema. Findings were characteristic of an infectious spondylitis. There was prevertebral edema, but no obvious collection.
She was referred for a CT guided biopsy a month later.
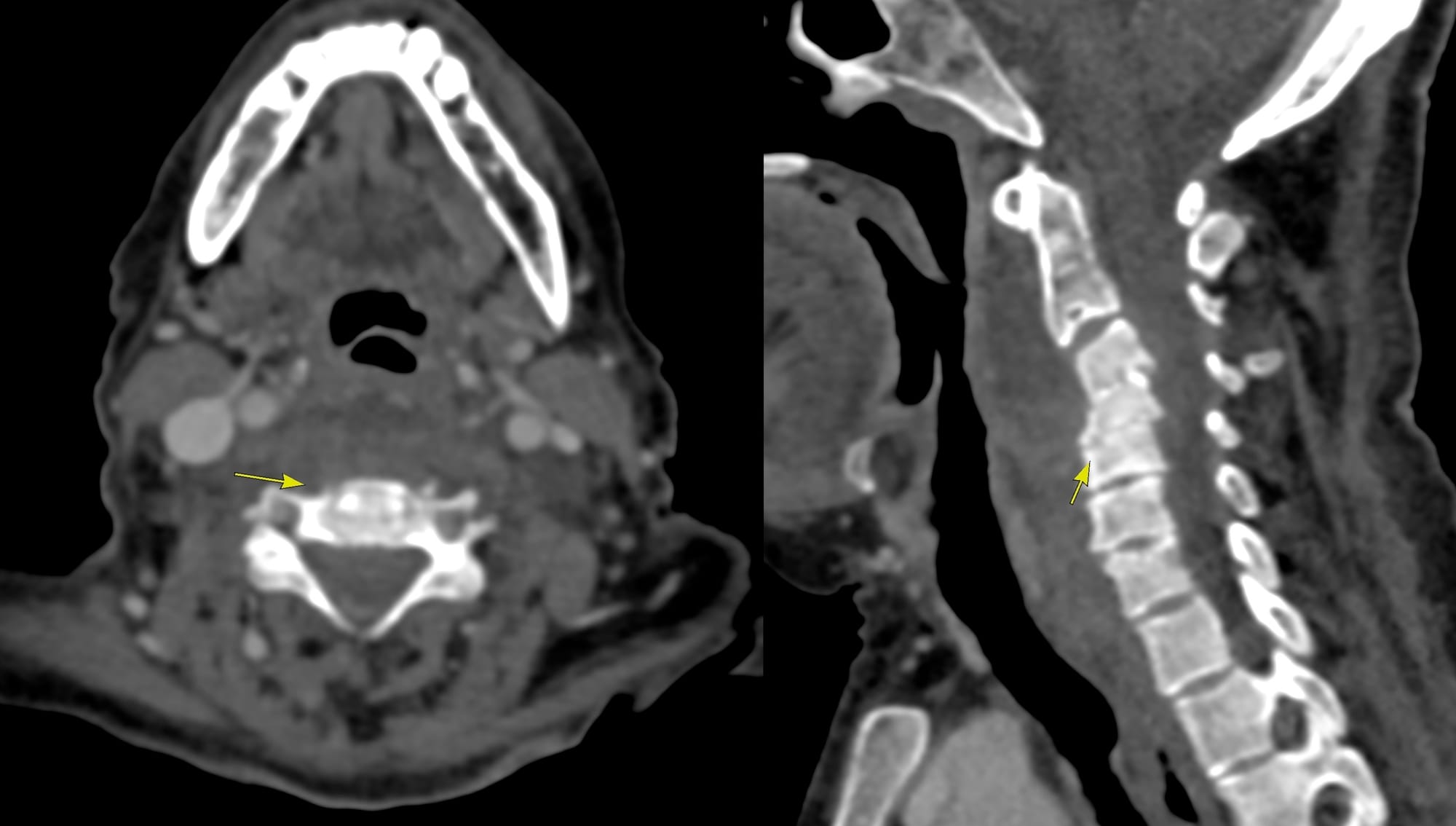
During the counseling session, 3 days prior to the biopsy, a contrast CT scan showed progression of disease with involvement of C4-5 and increase in the prevertebral soft tissue, but without an obvious collection (Fig. 2).
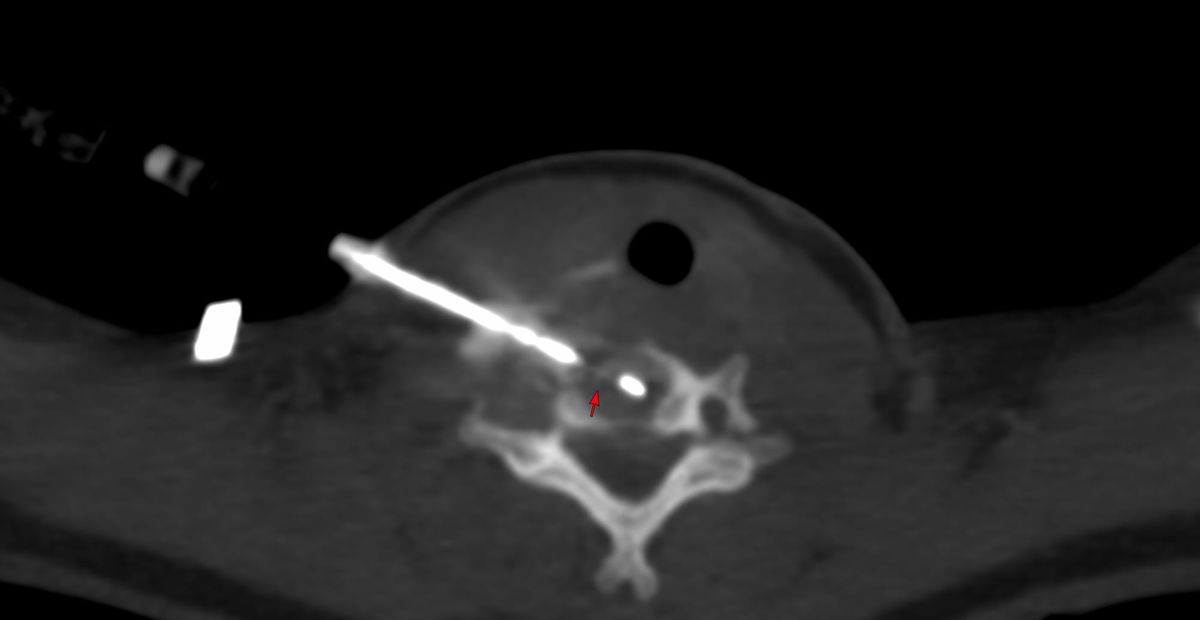
Of all the approaches possible, the retrocarotid approach which I had demonstrated earlier in a patient with a C3 plasmacytoma (Fig. 3) seemed to be the most ideal.
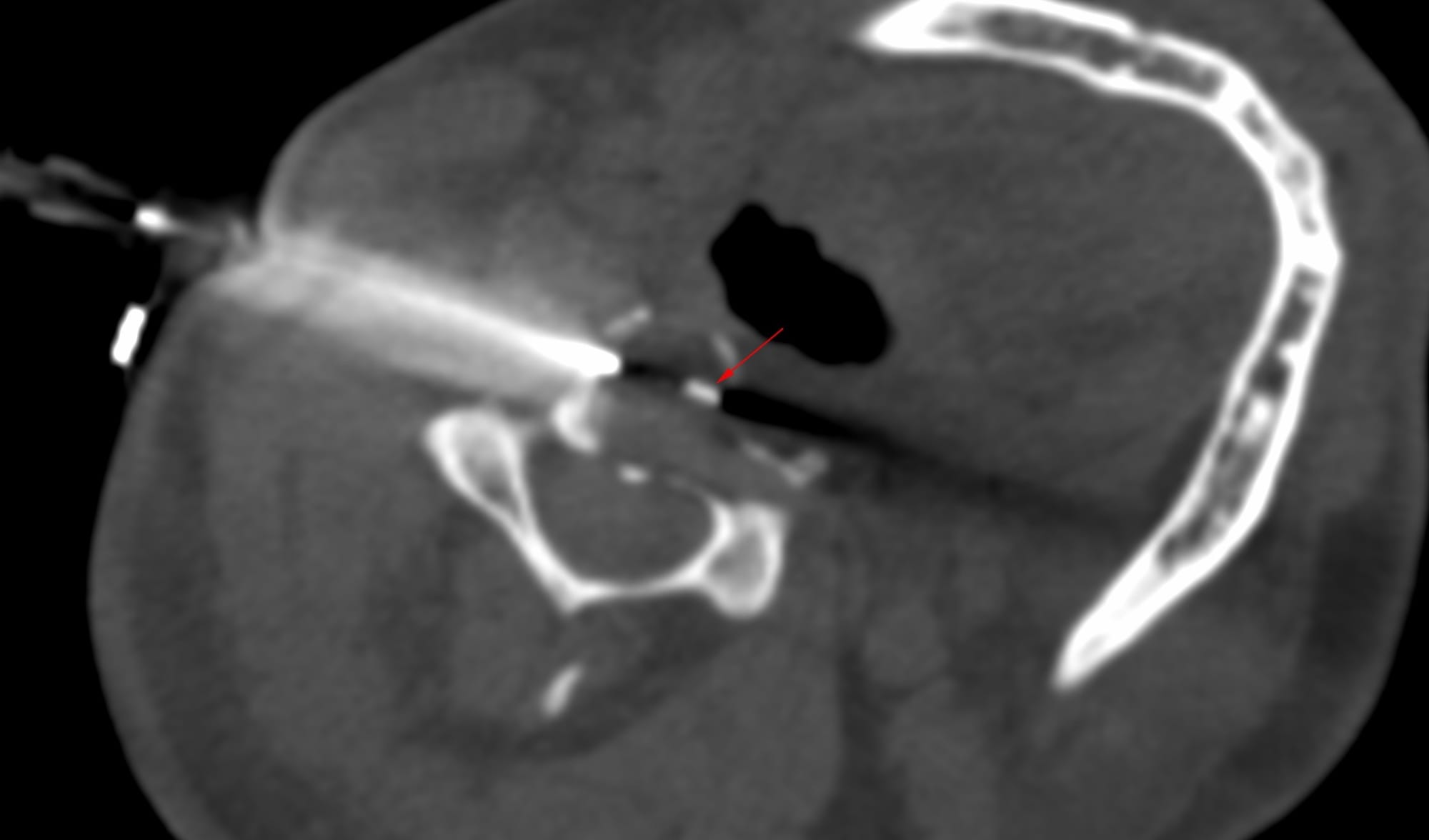
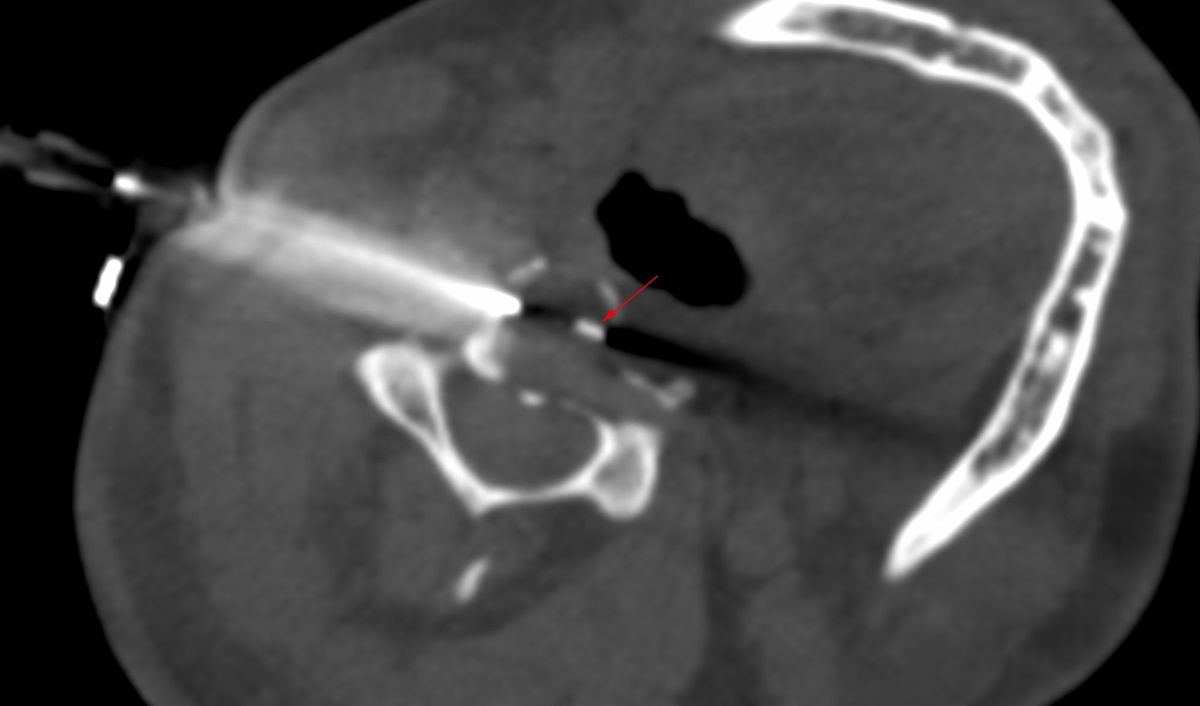
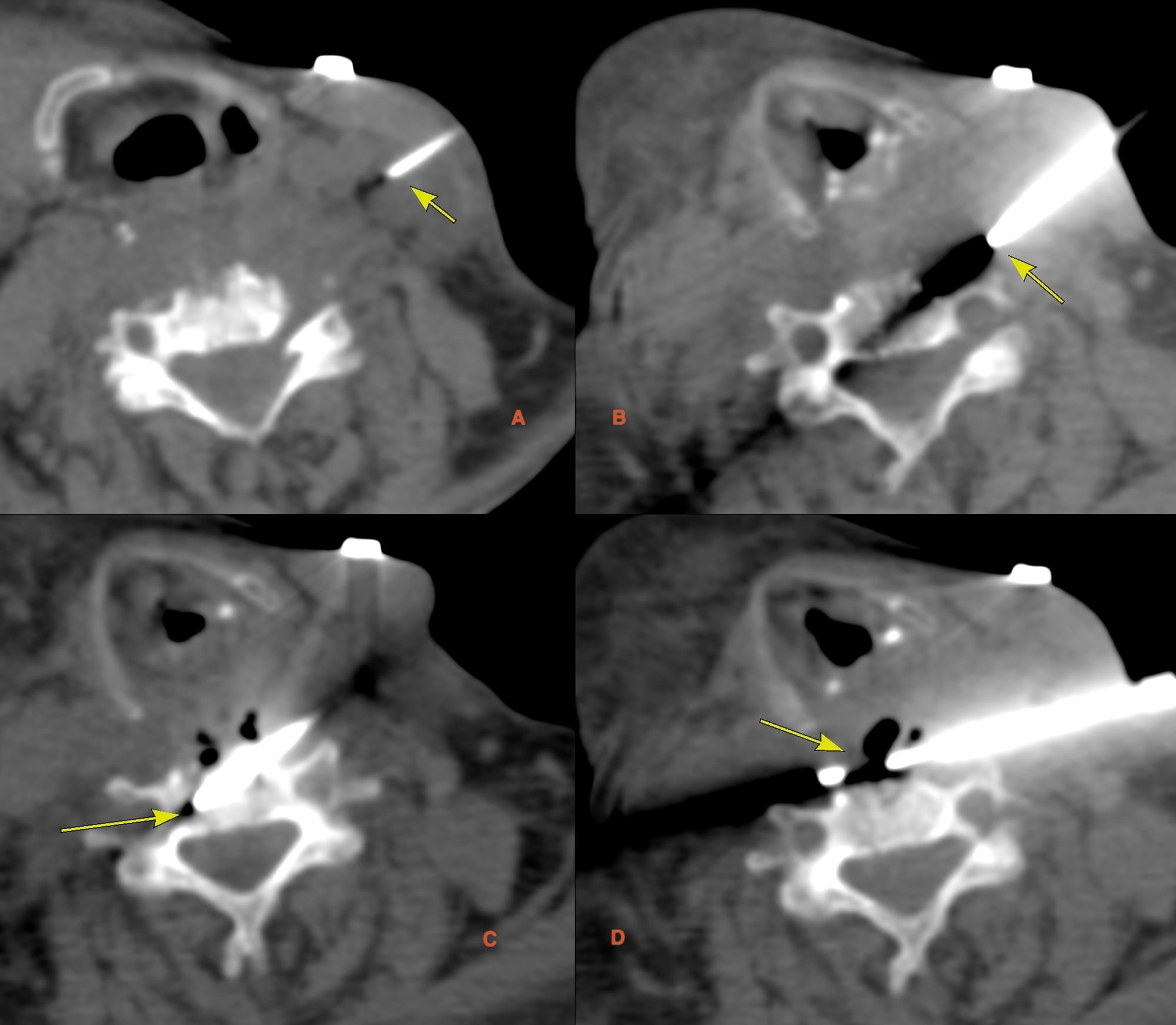
Fig. 4 and the video show how the biopsy was done. A coaxial 18G BARD biopsy gun was introduced from the left with the head turned to the right as much as possible (Fig. 4), posterior to the carotid vessels (A). Once the needle went past the vessels (B), then the navigation was simple. It was first pushed into the C3-4 disc (C) and a blood aspirate was obtained. The needle was then repositioned in the prevertebral space (D) and aspiration and biopsy were performed. Air is seen in the prevertebral soft tissue, but there was no pus.
Video
The procedure took 17 minutes without sedation with two cores for histopath and 4 for microbiology along with the aspirate for microbiology.
The final diagnosis was E.coli infection.
Region: Cervical Spine
Age: 72 years
Findings: Progressive C3 to C5 infectious spondylitis
Lesion Biopsied: C3-4 disc and prevertebral soft tissue
Size of Lesion: -
**Gun:**18G BARD, long, 20 mm throw, used 10 mm with hub
No of cores: 2 for HP and 4 for micro along with aspirate for micro
Sedation: No
Position & Approach: Supine
Time Taken (marker to wash-out): 17 mins
Complication: None
Level of Difficulty: 4/5
Diagnosis: E.coli infectious spondylitis
I have also discussed the retrocarotid approach in lower cervical spine lesions.
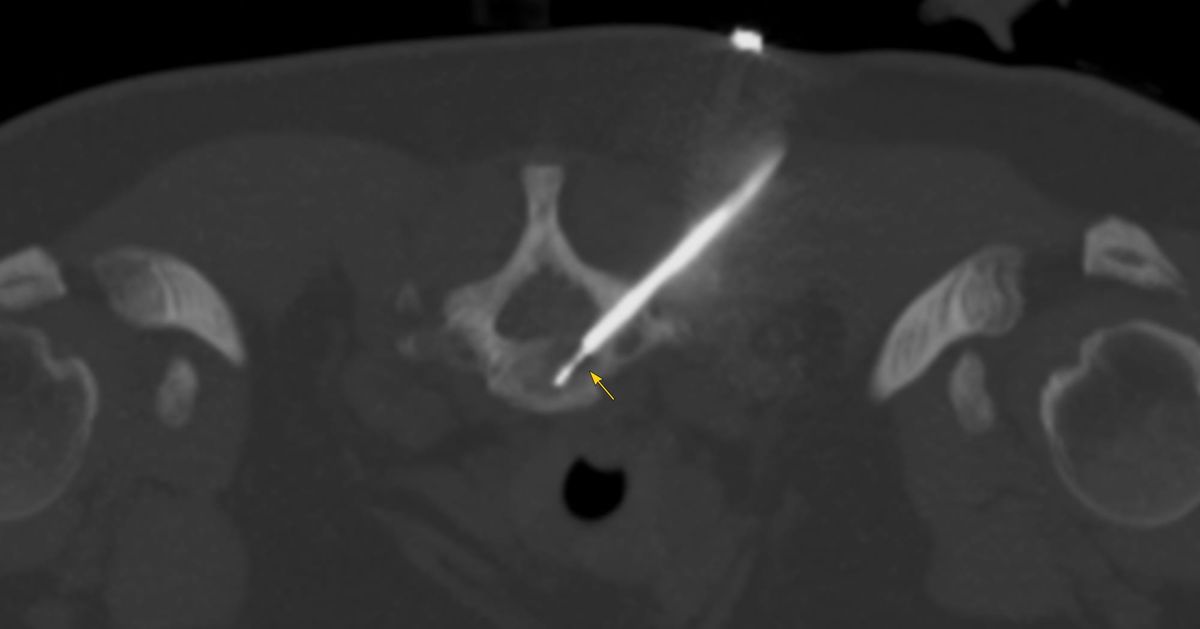
A careful evaluation of the images, often yields a safe route - from supine transthyroid to retrocarotid to prone transpedicular as this list of cases at www.ctbiopsy.com shows (Fig. 5).
Different Cervical Spine Biopsies

Index and Table of Contents
174 Cases with Videos
10 Cases with Images (With or Without Short Videos)
2 Snippets
5 Lectures
4 Cases of the Day (CODs)
New Onetime Lifetime Subscription
 Bhavin Jankharia
Bhavin Jankharia
Previous Posts:
Other Sites and Cases:
Case of the Day on YouTube
{kind=link}