
Radiologists need to up their game and do more of these biopsies...while they still can.
Current Case:
71-years old man operated for renal cell carcinoma (RCC) had a surveillance CT showing multiple small lung nodules. He was referred for a CT guided biopsy.
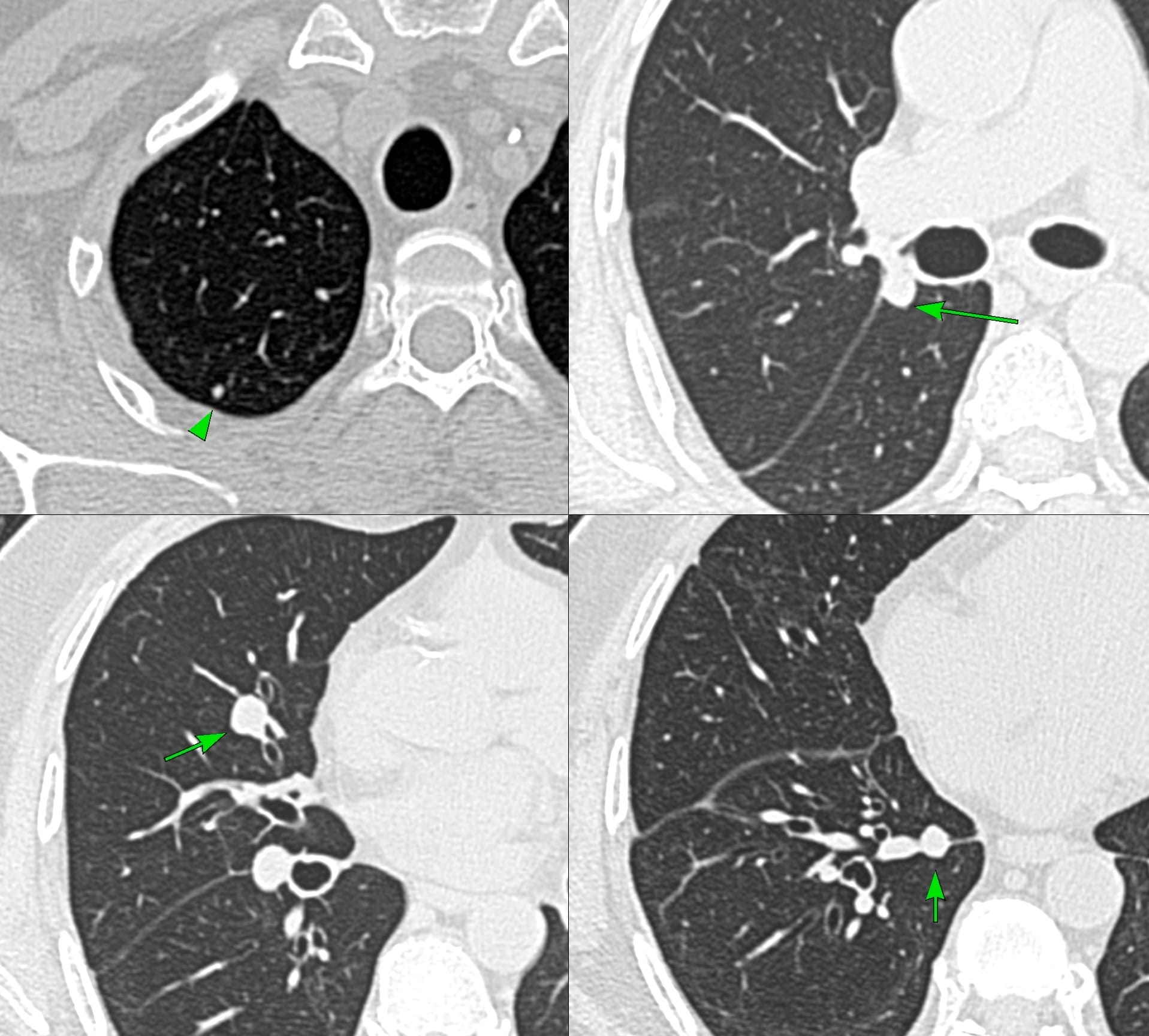
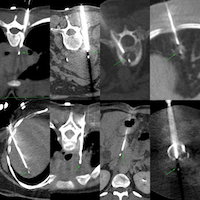
Fig. 1 shows the right sided lung nodules. Of all of these the right lower lobe nodule in the medial basal segment seemed the easiest and simplest.
The nodule measured an average of 8.5 mm in size - 9.2 mm along the z axis and 253 cu mm (Fig. 2).
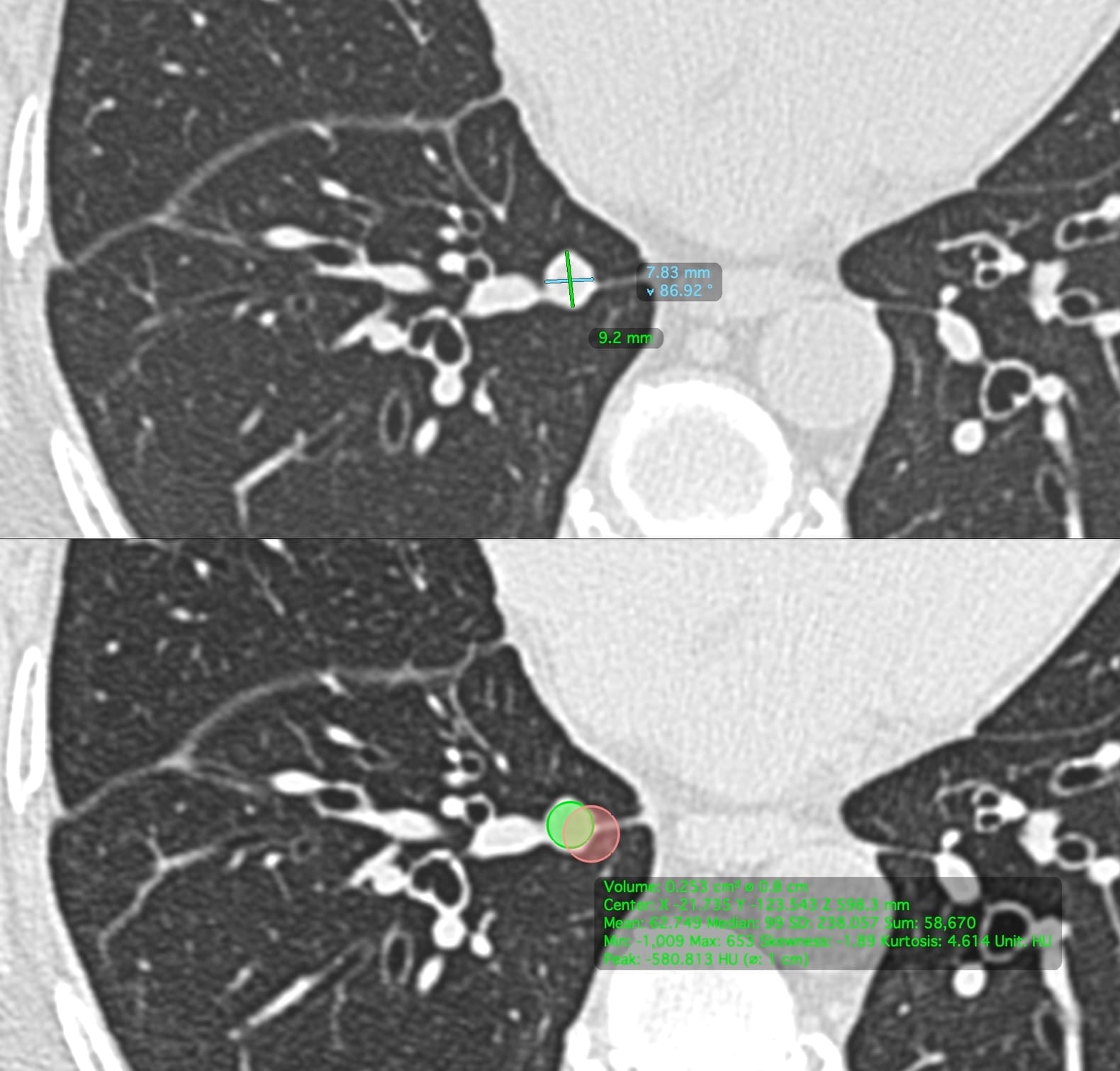
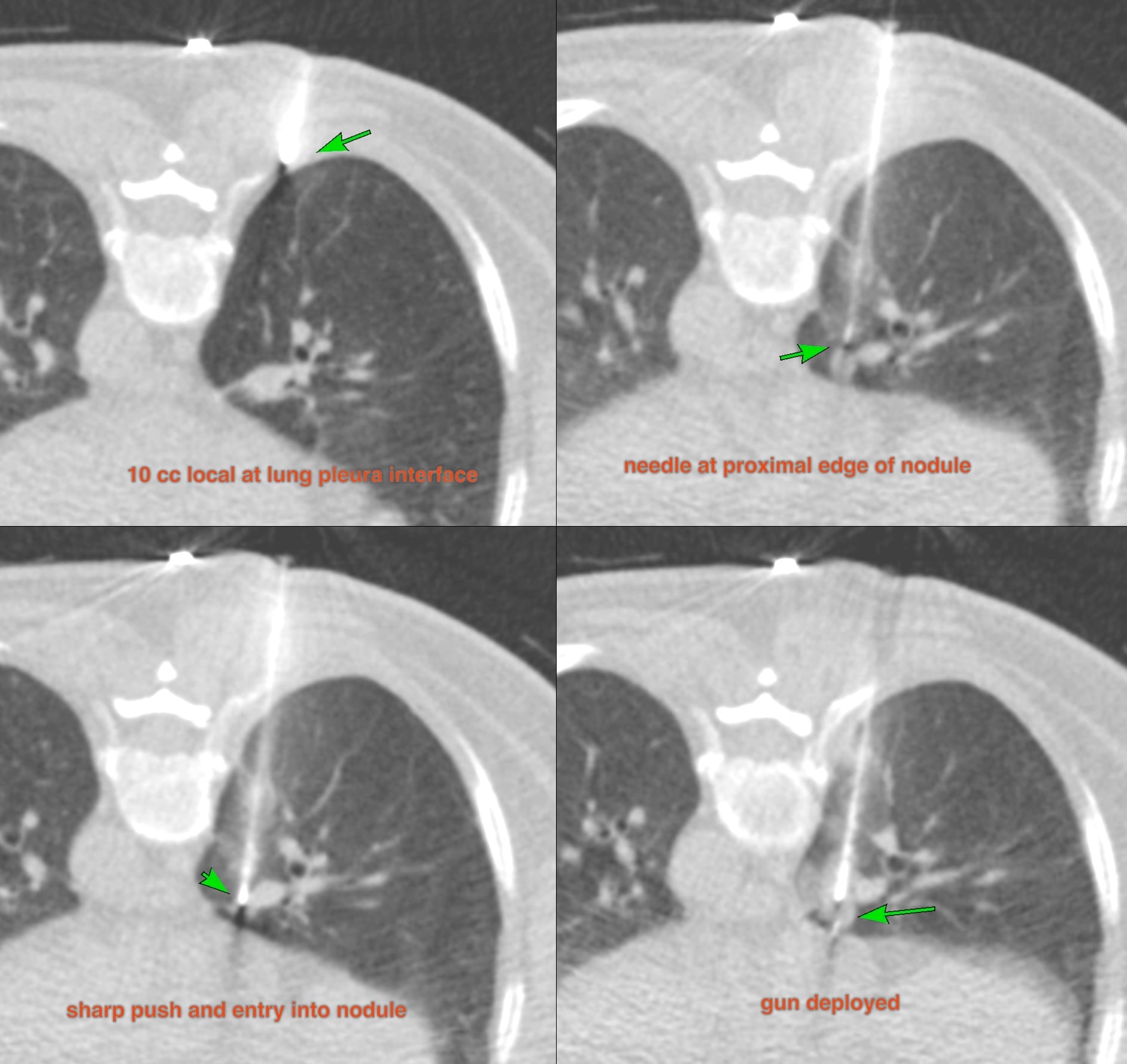
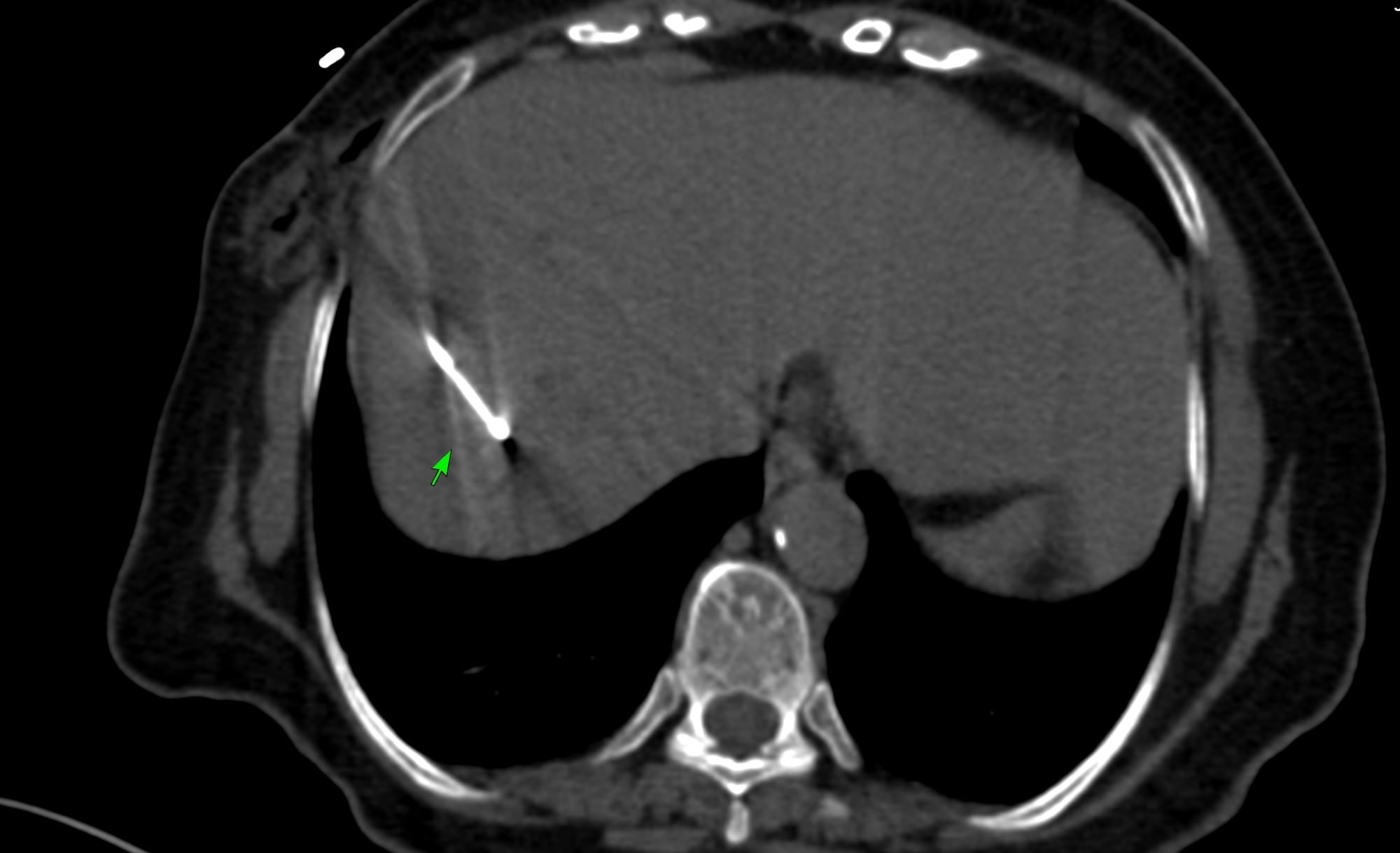
Fig. 3 and the YouTube video show the biopsy. A 20G Cook needle was first introduced up to the lung-pleura interface and 10 cc of lignocaine was injected. Then the needle was advanced up to the proximal edge of the nodule, which was then pierced with a quick jab and the gun was deployed. The tray deployment was kept at 6-8 mm to avoid overshooting, but there was still some overshooting as the image shows. Four cores were obtained only for histology in 11 minutes.
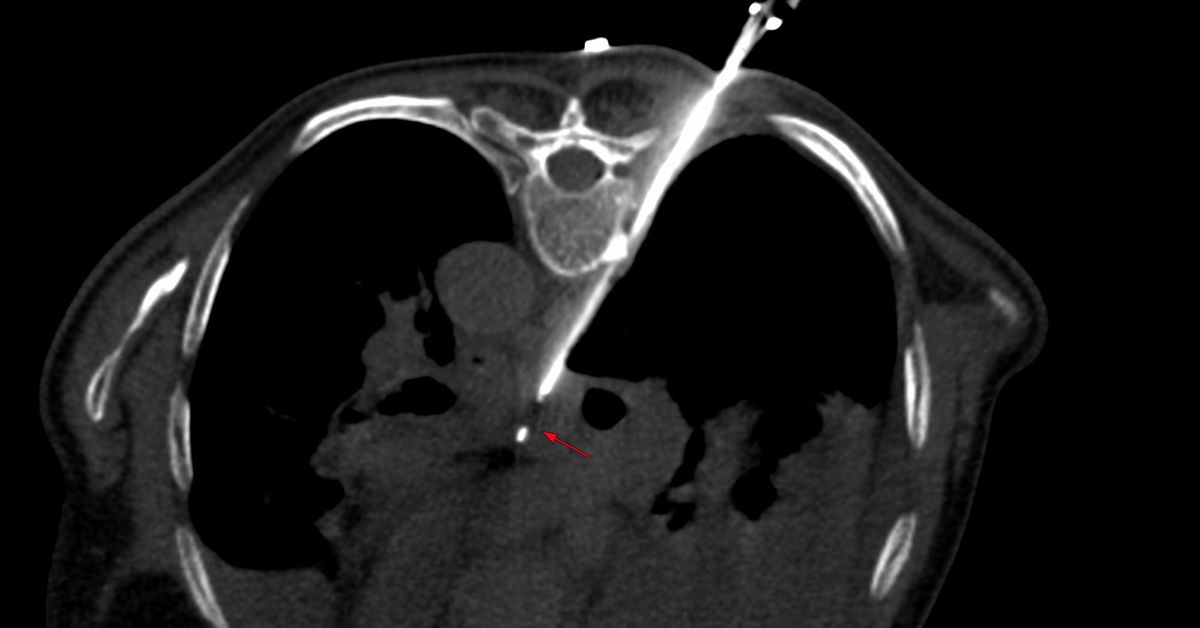
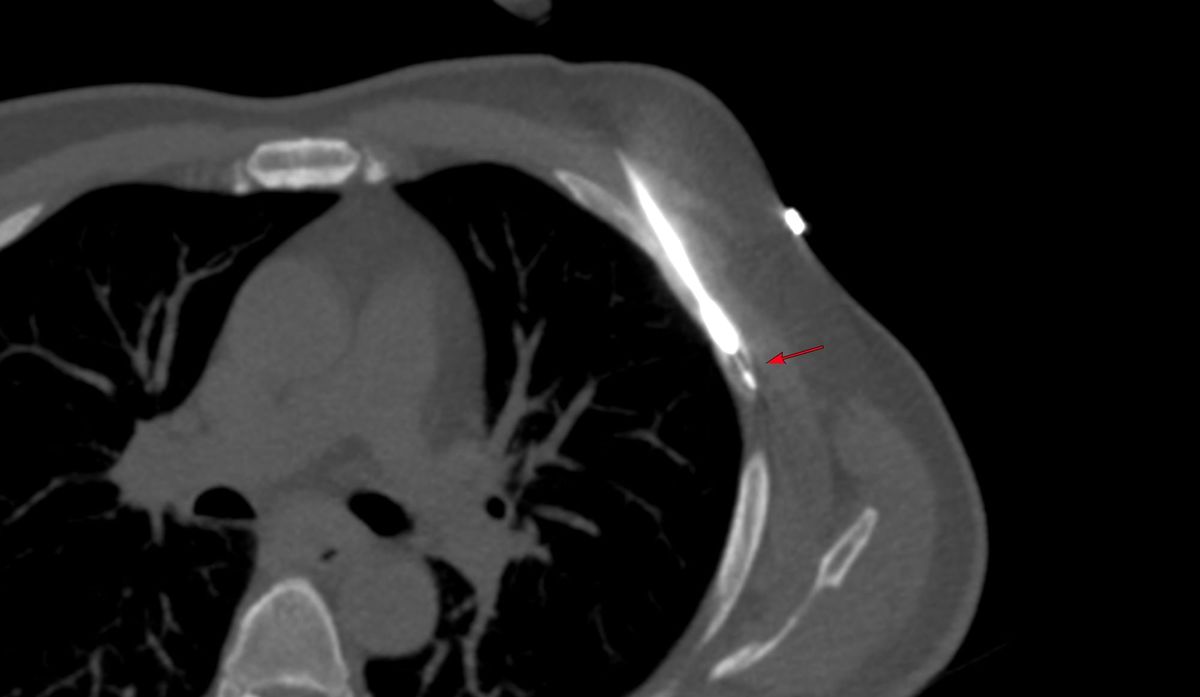
The rapid rollover (Fig. 4) showed mild perilesional hemorrhage. The patient did not have hemoptysis. The 6 mins check scan showed a 5-10 cc pneumothorax. As per protocol, the patient was kept supine for a hour a repeat scan showed no change and he was then allowed to leave with complete bed rest mandated for 24 hours.
The final diagnosis was metastasis from renal cell carcinoma.
Region: Lung
Age: 71 years
Findings: Multiple lung nodules
Lesion Biopsied: Nodule in medial basal segment right lower lobe
Size of Lesion: 9.2 mm z axis x 7.8 mm - avg 8.5 mm - vol 253 cu mm
Gun: 20G Cook, 10 mm throw, long
No of cores: 4 for histopath
Sedation: None
Position & Approach: Prone
Time Taken (marker to wash-out): 11 mins
Complication: Hemorrhage mild to moderate and 10 cc pneumothorax
Level of Difficulty: None
Diagnosis: Metastasis from renal cell carcinoma
Many radiologists refuse these biopsies as was the case in the primary institution where he was treated. These are not difficult. While some experience and expertise is needed, with a little focus, it is usually possible to find a safe route into the nodule. The trick is to get to the proximal edge and then with one sharp jab pierce the nodule and not to overshoot with the gun.
Since radial EBUS is now being used for such nodules and has been considered non-inferior, and given the short memory that physicians have, if I post something similar 10 years from now, I am sure to get blowback (as I got for the subcarinal and paratracheal node biopsy posts) saying, this should only have been attempted using radial EBUS. People forget that before EBUS, all of these nodules were biopsied, safely, accurately and successfully by CT scan, including mediastinal nodes and masses.

Just because a new modality is available, does not mean it has to be come a de facto standard, just because the gatekeepers now have access to the modality before the patient is sent to the radiologist.
Different CT Guided Biopsy Small Nodule Lung Biopsies
Index and Table of Contents
174 Cases with Videos
8 Cases with Images (With or Without Short Videos)
2 Snippets
5 Lectures
4 Cases of the Day (CODs)
New Onetime Lifetime Subscription
 Bhavin Jankharia
Bhavin Jankharia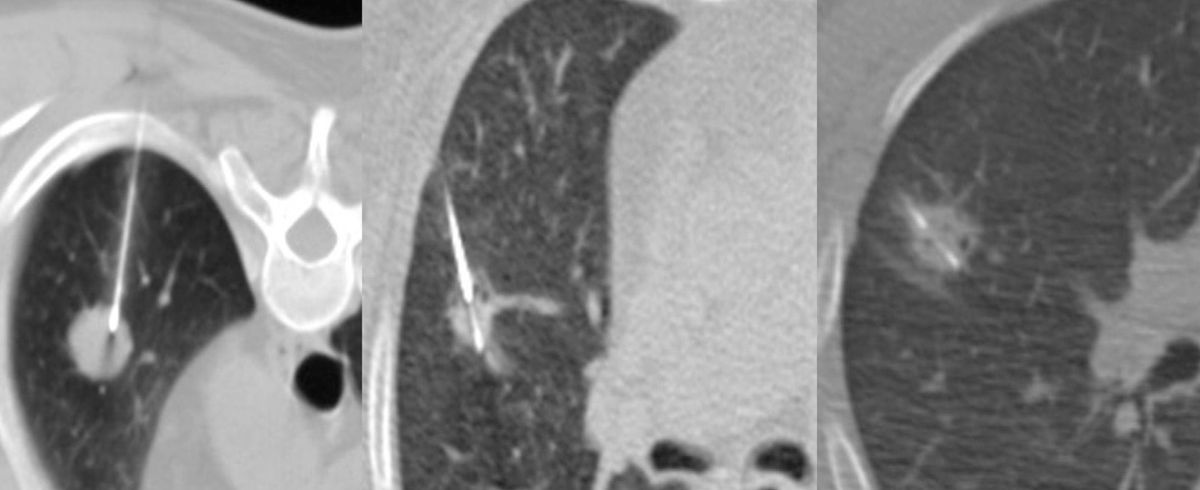
Table of Contents
Previous Posts:
Other Sites and Cases:
Case of the Day on YouTube
{kind=link}